Abstract
Coexistence of symptomatic coronary artery disease(CAD) and significant carotid artery stenosis(CAS) ranges from 3.4% to 22% . Although a simultaneous carotid endarterectomy and coronary artery bypass is generally accepted, there are discussions about the best approach. The difference in our case was the coexistence of coronary artery disease with internal carotid artery stenosis instead of a right common carotid artery stenosis, which was unsuitable for stenting. In this study, we report a simultaneous coronary artery bypass and an aorta-right common carotis artery bypass operation with a synthetic graft in a patient with carotid artery disease and coronary artery disease.
Keywords :
Coronary artery disease
, Coronary artery bypass grafting
, Carotid artery stenosis
Turkish Abstract
Semptomatik koroner arter hastalığı ve belirgin karotis arter lezyonu birlikteliği oranı %3,4 ile %22 arasındadır. Genel olarak tek bir operasyonda iki girişimin bir arada yapılması kabul görse de en iyi yaklaşım hala tartışmalıdır. Sunulan vakanın farkı ise koroner arter hastalığı ile birlikte olan karotis arterindeki lezyonun karotis interna yerine sağ karotis komunis arterinde bulunması ve stent girişimine uygun olmamasıydı. Bu olguda, karotis arter ve koroner arter hastalıkları bir arada olan ve eş zamanlı olarak koroner baypas operasyonu ile sentetik greftle aorta ve sağ karotis komunis arteri arasına yapılan baypas operasyonu sunulmuştur.
Turkish Keywords :
, Koroner arter hastalığı
, Koroner arter baypas operasyonu
, Karotis arter darlığı
Introduction
Coexistence of symptomatic coronary artery disease(CAD) and significant carotid artery stenosis(CAS) ranges from 3.4% to 22% ¹. Hertzer et al. reported that 28% of patients with extracranial cerebrovascular disease had severe correctable CAD ². Although asimultaneous intervention in during one general anesthetic session is generally accepted, there are discussions about the best approach ³. However, we chose a simultaneous approach for our case with coexisting right common carotid artery stenosis and coronary artery disease in which the carotid artery stenosis was unsuitable for endarterectomy or carotid stenting. In this study, we reported a patient with carotid and coronary artery disease that we performed a sımultaneous coronary artery bypass and ascending aorta-right common carotid artery bypass with synthetic graft.
Case Report
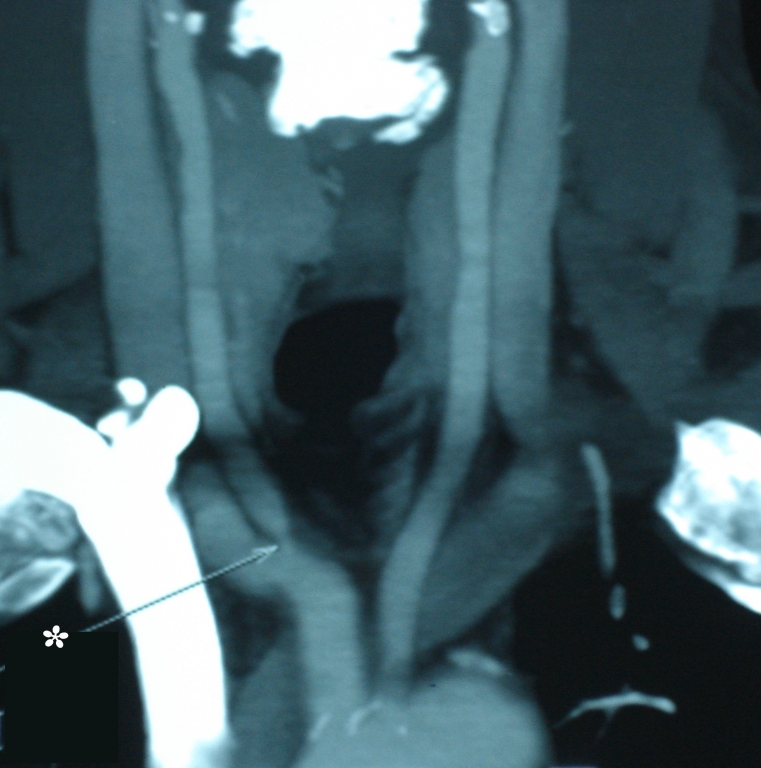
A 56 year-old man, who had unstable angina pectoris and recurrent amaurosis fugax was referred to our clinic. In the physical examination, a murmur over the right carotid artery was noticed. He had no comorbidities or risk factors for atherosclerotic cardiovascular disease except for being a smoker. Coronary angiography and a computed tomographic angiography (CTA) for carotid arteries were performed. The coronary angiography showed critical lesions in the left anterior descending artery (LAD) and second diagonal branch(D2), right coronary artery(RCA) and circumflex artery branches. The carotid artery CTA showed a critical osteal stenosis in right common carotid artery which was not unsuitable for stenting or endarterectomy (Figure 1A).
As result, we made a decision to perform a simultaneous coronary artery bypass and ascending aorta-right carotid artery bypass grafting. Under general anesthesia a median sternotomy was performed, then the left internal mammarian artery (LIMA) and saphenous vein graft were harvested and prepared. After systemic heparinisation, a standart aortacaval canulation was completed and the skin incision was extended towards the right carotid artery trace. Endarterectomy was not considered due to the difficulty of complete endarterectomy because of the anatomic localisation of the lesion and the embolisation risk of an incomplete endarterctomy. Vascular cross clamps were placed in the right common carotid artery proximally and distally beyond the atherosclerotic segment while patient?s blood pressure was kept between 120-140 mmHg. Ascending aorta-right common carotid bypass with a 6 mm ringed polytetra flouro ethylene (PTFE) grafting (figure 1B) was performed in end to side fashion. Carotid shunt was not used.
After the right common carotid artery blood flow had been restored and cardiopulmonary bypass was started, coronary artery bypass graftings (Aorta-PDA,Aorta-OM1-OM2 sequential, Aorta-D2, LIMA-LAD) were performed. After an eventless postoperative period of 7 days, the patient was discharged. The control examinations in postoperative 1. and 3. months showed a patent graft.
Discussion
The coexistence of a carotid artery and a coronary artery disease is one of the major pathologies in cardiovascular surgery. However, the screening of all asymptomatic population for carotid stenosis is an inefficient and expensive strategy. On the other hand, carotid artery stenosis is the most common cause of stroke and atherosclerosis and has a role in one third of all strokes . Also, the risk of stroke in CABG patients with bilateral hemodynamically significant carotid artery stenosis could be considerably higher . Follow-up of carotid endarterectomy (CEA) patients often reveals myocardial infarction as a common cause for late deaths. Hertzer and Arison found that 37% of late deaths after CEA were secondary to myocardial infarction 4. The increased incidence of myocardial infarction after carotid endarterectomy and increased neurological events after coronary surgery shows the relation between these two diseases. Commonly, these discussions take place when there is a coexistence of internal carotis stenosis and coronary artery disease. Char et al. emphasize that patients undergoing combined CAB/CEA enjoy excellent long-term freedom from stroke, as well as a good long-term survival 5.
Clinical examination, doppler ultrasound and arteriography are enough for the diagnosis of these cases. The presence of sufficient collateral circulation of the contralateral carotid artery and vertebral arteries as a result of slowly developing atherosclerosis in the common carotid artery causes weak sympthoms. With its major neurological complications like stroke and death and with its socioeconomic harm, carotis artery stenosis are one of the most important health problems. Especially in cases with significant carotid stenosis and coronary artery disease, the high rate of neurological complications increases the importance of simultaneous intervention. The management of cardiac surgery in patients with carotisd artery stenosis is contested 6. The first simultaneous intervention was described in 1972 by Bernard et al 7. Mackey et al. suggested three different ways for the management of surgery 8. Those are simultaneous, staged and reverse staged interventions, but there is no consensus on the interventions yet. In general, the incidence of postoperative stroke after CABG ranges from 0.7% to 5% 9. Coronary revascularization operations with a carotid stenosis have an increased risk of postoperative stroke. The incidence of stroke in patients with no diagnosis of carotid disease undergoing cardiac surgery is 0.2% to 8% according to the patient?s age 10. Coronary revascularization in a patient with internal carotid artery stenosis more than 50% is associated with a postoperative stroke rate of 6%, which increases significantly to more than 16% when stenosis is more than 90% ¹¹. Also, stroke after coronary bypass increases the risk of mortality to 1-3% ¹². Likewise, some studies showed that coronary artery bypass surgery performed without any intervention on carotids in cases with significant carotid stenosis have a neurological event and a mortality rate between 7.4 - 20.3% and 6.9 - 13.8% respectively13. The high morbidity and mortality rates increased the importance of simultaneous approaches. As a result, we decided on performing a simultaneous approach on our patient.
To decrease mortality and neurological morbidity rates, simultaneous surgery in coronary and common carotid artery lesions is important. Simultaneous operations should be considered in patients with significant carotid and symptomatic coronary artery disease even if the carotid lesion is atypical and an endarterectomy is unfeasible.
References
- Mackey WC, Khabbaz K, Bojar R, et al. Simultaneous carotid endarterectomy and coronary bypass: perioperative risk and long-term survival. J Vasc Surg 1996;24:58? 64.
- Hertzer, N. R. Young, J. R., Beven, E. G, et al. Coronary angiography in 506 patients with extracranial cerebrovascular disease. Archives of Internal Medicine 1985;145:849?852.
- Çiçekçioğlu F, Parlar AI, Altınay L, Yay K, et al. Successful coronary artery bypass grafting in a patient with bilateral internal carotid artery occlusion: a case report. Turkish J Thorac Cardiovasc Surg 2010;18:318-320.
- Hertzer N. R, Arison R. Cumulative stroke and survival ten years after carotid endarterectomy. Journal of Vascular Surgery 1985; 2: 661?668.
- Char D, Cuadra S, Ricotta J, Bilfinger T, Giron F, et al. Combined coronary artery bypass and carotid endarterectomy: long-term results. Cardiovasc Surg 2002;10:111?115 .
- Biçer M, Çokünlü O, Saba D, Yanar M, et al. Early results of combined and staged carotid endarterectomy with beating heart coronary artery bypass surgery. Uludağ Medical Journal 2007; 33:135-139.
- Bernhard VM, Johnson WD, Peterson JJ. Carotid artery stenosis: Association with surgery for coronary artery disease. Arch Surg 1972;105:837-40.
- Mackey WC. Carotid and coronary disease: Staged or simultaneous management. Semin Vasc Surg 1998:11:36- 40.
- Baiou D, Karageorge T, Spyt T, Naylor AR. Patients undergoing cardiac surgery with asymptomatic carotid stenoses have a low risk of peri-operative stroke. Eur J Vasc Endovasc Surg 2009;38:556-5
- Gardener T. J, Horneffer P.J, Manolio T. A. et al. Major stroke after coronary artery bypass surgery: changing magnitude of the problem. J Vasc Surg 1986;3:684-7.
- Faggioli GL, Curl GR, Ricotta JJ, et al. The role of carotid screening before coronary artery bypass. J Vasc Surg 1990;12:724?31.
- Loop FD, Lyte BW, Cosgrove et al. Coronary artery bypass graft surgery in the elderly: indication and out come. Cleve Cl. J Med 1998; 55:23-4.
- Gansera B, Schmidtler F, Weingartner j, Kiask T, et al. Simultaneous carotid endarterectomy and cardiac surgery: early results of 386 patients. Thorac Cardiovasc Surg 2012;60:508-16
Information Presentation
Yazımız 8. Kardiyoloji ve Kardiyovasküler Cerrahide Yenilikler Kongresinde poster olarak yayınlanmıştır.
|