Abstract
The ultrasonography (USG) and magnetic resonans imaging (MRI) findings of a 52-year-old woman with primary lymphomatous involvement of the left brachialis muscle are discussed. Multimodality imaging and familiarity with the presentation and imaging features of skeletal lymphoma can play an important role in the differential diagnosis and prediction of lymphoma. USGguided biopsy led to establishing a correct diagnosis in this patient.
Keywords :
Skeletal lymphoma
, Ultrasound
, Magnetic resonance imaging
Turkish Abstract
Bu yazıda, sol brakiyalis kasında primer lenfomatöz tutulumu olan 52 yaşındaki kadın hasta, ultrasonografi (USG) ve magnetik rezonans (MRG) görüntüleme tetkikleri ile elde edilen bulguları ile birlikte sunulmaktadır. Multimodalite görüntüleme ve iskelet lenfomasının prezentasyon şekli ve görüntüleme bulgularının bilinmesi ayırıcı tanıda ve lenfoma ön tanısında önemli rol oynamıştır. USG kılavuzluğunda gerçekleştirilen biyopsi tanıya ulaşılmasını sağlamıştır.
Turkish Keywords :
, İskelet lenfoması
, Ultrasonografi
, Manyetik rezonans görüntüleme
Introduction
Primary lymphoma of the skeletal muscle is a rare occurrence accounting for 0.5% of all extra-nodal lymphomas and mainly consists of B-cell non-Hodgkin type (NHL) (> 95%) 1-4. Magnetic resonance imaging (MRI) is often the initial imaging modality of choice in musculoskeletal lymphomas and MRI findings are widely described in the literature in contrast to ultrasonography (USG) which is also a useful imaging tool regarding muscular diseases 5-7.
Herein, we present a patient with primary skeletal muscle lymphoma involving the brachialis muscle of the upper extremity. The initial imaging study was USG and the differential diagnosis was based upon USG findings with lymphoma as the leading diagnosis. USG-guided aspiration biopsy confirmed the presence of lymphoma. MRI was later carried out to rule out bone involvement and metastatic disease. Our primary aim was to discuss the USG and MRI findings of this rare skeletal muscle lymphoma.
Case Report
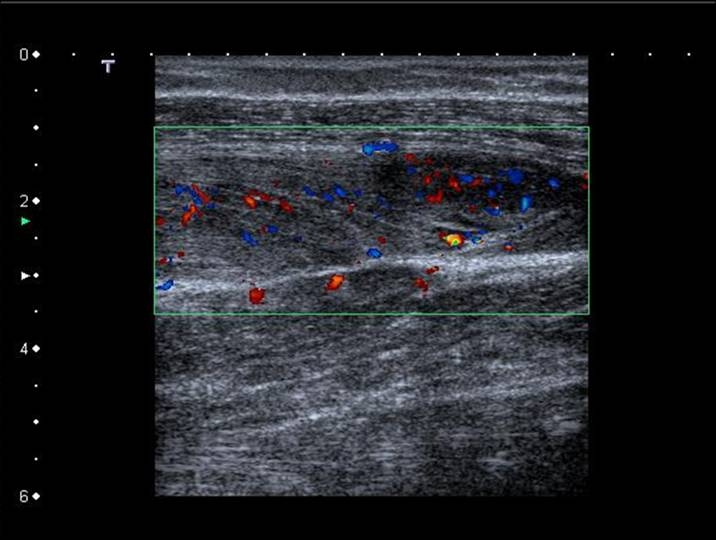
A 52-year-old woman presented pain and swelling of the left arm. The pain started after a trivial injury nearly a year ago and she did not recall any major trauma to her arm and she was not involved in sports actively. Her pain gradually increased in intensity and she noticed swelling in her left lower arm near the antecubital fossa nearly a month ago. On palpation, a diffuse, hard lump was noted proximal to the elbow anteriorly which was quite tender. She had mild anemia and leukocytosis with no fever. Erythrocyte sedimentation count was elevated with a mild increase in LDH. HIV and hepatitis serology were negative. An USG study was done which showed a diffusely thickened brachialis muscle with decreased mildly heterogeneous background echogenicity; the fibrillary structures however were brightly echogenic and were in a relatively disorganized architecture as compared to the contralateral muscle. Additionally, lobular and well defined hypoechoic areas were depicted within the muscle, which were hypervascular on Doppler imaging with decreased vascular resistance on spectral analysis (Figure 1).
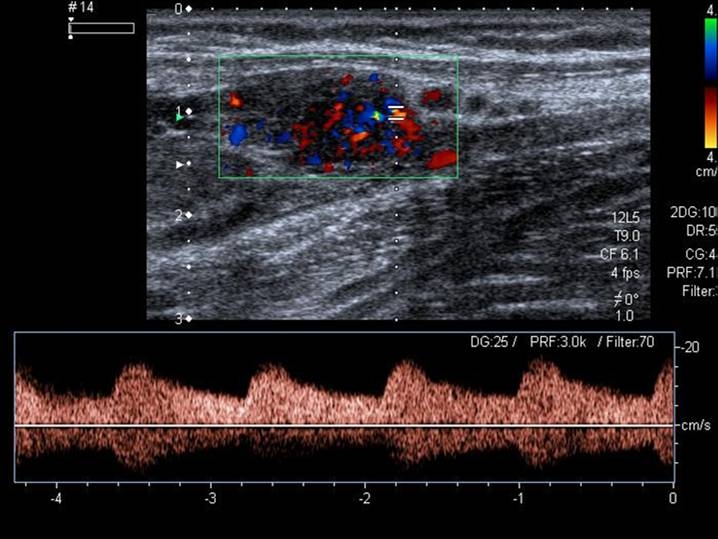
Doppler imaging revealed increased vascularization of the entire muscle as compared to the adjacent and contralateral muscles (Figure 2).
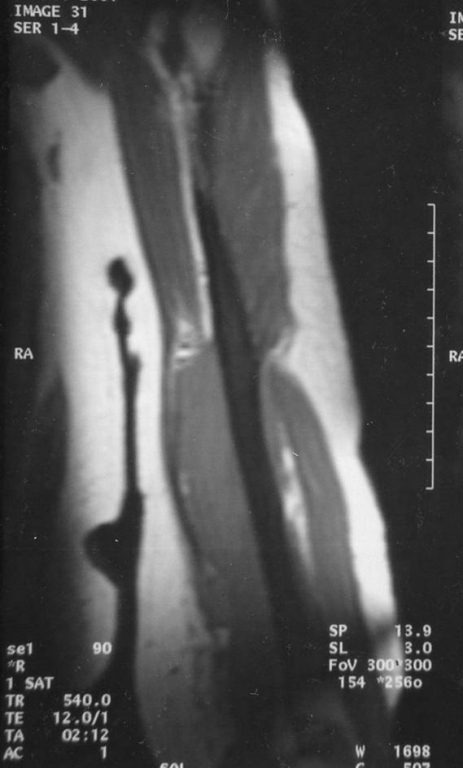
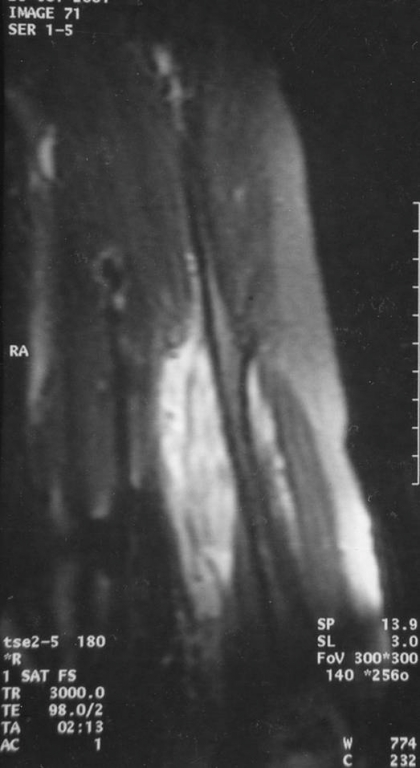
No venous or arterial occlusion was demonstrated. Hypoechoic, small nodular lymphadenopathies adjacent to muscle along with diffuse thickening of the subcutaneous tissues anteriorly and prominent echogenic fat stranding were also evident. This pattern suggested either an infiltrative or an inflammatory pathology. Lymphoma was primarily suggested and included in the differential diagnosis. This pattern was confirmed with MRI as well. These lesions were hyperintense on T2 weighted (T2W) images (Figure 3A) and hypointense on non-contrast enhanced T1W images (Figure 3B).
Contrast enhancement of the entire brachialis muscle with intramuscular masses was seen, which clearly outstood on contrast enhanced T1W images (Figure 4). No lesions were detected involving the humerus.
An USG-guided aspiration biopsy of the muscle was performed and the cytopathologic examination suggested presence of lymphoma. The patient underwent excisional biopsy and histopathology revealed a high grade of NHL, rich in B lymphocytes. Bone marrow biopsy revealed a normocellular marrow with no evidence of lymphoma. Additional imaging studies were done which excluded involvement of other sites. The patient was classified as stage IE NHL according to Ann-Arbor classification and received 6 cycles of cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone (CHOP) and rituximab chemotherapy regimen and was in complete remission four years after her initial diagnosis.
Discussion
The common clinical scenario in lymphomatous involvement of the muscle is often secondary hematogeneous dissemination from nodal disease elsewhere or adjacent extension from an involved site. Primary extranodal lymphomatous involvement is exceedingly rare (0.1 % of all lymphomas) 2,4-7. In a study by Travis et al 2 only eight cases of primary skeletal muscle lymphomas were found over a 10-year period among 7000 malignant lymphomas and in a 2002 review by Masaoka et al 8 only 7 skeletal lymphoma cases were reported so far in the upper extremity. In another review, no lymphoma cases were detected among skeletal muscle tumors during a 21-year period 9,10. But a recent overall increase in incidence is noted related to the HIV epidemic, immunosupression and drug abuse 8,11.
The most commonly involved sites are the upper and lower extremities including the thigh, calf and upper arm 5,8. The average age of presentation is usually around 60- 70 years of age and a preceding trauma history is often present 3. Also a preceding rippling muscle syndrome is described where percussion induces muscle mounding, rippling and serum creatine kinase elevation 12.
Skeletal muscle lymphoma either manifests as focal mass/masses in the muscle or diffusely enlarges the muscle preserving the fibrillary structure and intermuscular fat planes. Lymphoma can also present a mantle of soft tissue that insinuates along myofacial planes into the deep muscle compartments without muscle invasion. This type of involvement where muscle structure and fat planes are preserved is indigenous to lymphoma 7,13. If muscle invasion occurs, often multiple compartments are affected, spanning a long segment of the extremity. Clinicians should be aware that compartment syndrome may develop in such a setting and paraneoplastic syndromes may exist as well inherent to the nature of lymphoma 8.
Subcutaneous infiltration occurs in approximately 100% of the cases, multiple compartment involvement occurs in 50% and neurovascular bundle invasion occurs in 30% of the cases 5. Involvement of the subcutaneous tissue overlying the lesion is prominent either in the form of extension, skin thickening, stranding or edema 5. In our case, USG was more successful in depicting subcutaneous tissue involvement. Significant hemorrhage and necrosis within or near the lesions has not been reported at all. Thrombophlebitis has been reported in only one case involving the lower extremity 4. The tumor may invade the adjacent bone and may metastasize to distant muscle segments 6,8. Significant cortical destruction may not be seen, marrow involvement is more probable 7.
These lesions are radiographically occult 7. On computed tomography (CT), the lesions are isodense with the muscle and may enhance with contrast medium. Occasionally no attenuation change may be seen on CT even with contrast administration; also, CT indications for muscular lesions are quite limited. CT therefore is not considered as a useful method for skeletal lymphoma imaging due to discursive findings 5,13,14. On MRI, the lesions are isointense in signal intensity on T1W images and high on T2W and there is avid Gadolinium enhancement. Fat suppression allows better visualization of tissue enhancement 13. USG is not used as widely as MRI in the diagnosis of soft tissue lymphoma. Chiou et al analyzed the USG findings of skeletal lymphomas; the lesions had homogenous hypoechogenicity with infiltrative margins with no anechoic spaces, consistent with rare occurrence of tumor necrosis. All were hypervascular with low resistance indices but no A-V shunts were noted. The lesions on USG were big masses such as nodal or confluent nodal, small nodal (<1 cm), disseminated, myositic and panniculitic. A striated appearance with homogeneous hyperechoic lobules of fat tissue, interspersed with tiny elongated hypoechoic strands, was the hallmark of panniculitic appearance, suggestive of lymphocytic infiltration 6. The same findings are also observed in our case.
The advantages of USG are its cost effectiveness, easy application, wide availability and ability to perform synchronous aspiration and biopsy procedures. USG allows not only assessment of muscle echogenicity and structure but also vascularization patterns 8. MRI is often the modality of choice in lymphoma due to its clear identification of anatomic relations, demonstration of bone lesions, and sensitivity to the presence of fat tissue or hemorrhage within the mass 13. However, MRI findings of lymphoma are not considered to be lesion specific 5,7.
Age of the patient and location of the mass are important in the differential diagnosis. The most common intramuscular masses in adults, that do not contain fat, are hematomas, soft tissue sarcomas and metastases; whereas in young patients, most common tumors are Ewing sarcomas, primary neuroectodermal tumors, eosinophilic granulomas and osteosarcomas 14,15. Benign inflammatory disorders such as pyomyositis (inflammatory or tuberculous), myopathies and osteomyelitis should also be considered. Skin involvement is common in inflammatory conditions but uncommon in sarcomas. Sarcomas tend to be compartmental, may contain hemorrhage and necrosis whereas lymphomas are infiltrative, may involve multiple compartments or invade the neurovascular bundle (with the exception of epithelioid sarcomas) 5.
Most skeletal muscle lymphomas (95%) are B-cell diffuse large cell type; T-cell types are much rarer 3,10. Surgery is not recommended because of high local recurrence, distant metastasis rates and disfigurement. There is often good response to chemotherapy as in our case but physicians should be cautious because sometimes, aggressive behavior may occur especially in certain T-cell types 4,8. MRI is recommended at frequent intervals for follow-up and monitorization 3. PET imaging may also be useful in this manner since skeletal muscle lymphoma is reported to be PET positive 4.
In conclusion, preservation of the muscle architecture, avid contrast enhancement, an infiltrative, multi-compartmental, insidious pattern of involvement with subcutaneous infiltration, neurovascular bundle invasion and absence of hemorrhage are the differentiating features of lymphoma well demonstrated by multimodal imaging, mainly USG and MRI.
References
- Glass AG, Karnell LH, Menck HR. The national cancer data base report on non-Hodgkin lymphoma. Cancer. 1997;80:2311-20.
- Travis WD, Banks PM, Reiman HM. Primary extranodal soft tissue lymphoma of the extremities. Am J Surg Pathol. 1987;11:359-66.
- Laffose JM, et al. A case of malignant primary non-Hodgkin?s lymphoma in skeletal muscle treated by exclusive chemotherapy. Joint Bone Spine. 2009;76:86-8.
- Alekshun TJ, et al. Skeletal muscle peripheral T cell lymphoma. J Clin Oncol. 2008;26:501-6.
- Suresh S, Saifuddin A, O?Donnel P. Lymphoma presenting as a musculoskeletal soft tissue mass: MRI findings in 24 cases. Eur Radiol. 2008;18:2628-34.
- Chiou HJ, et al. High resolution ultrasonography of primary peripheral soft tissue lymphoma. J Ultrasound Med. 2005;24:77-86.
- Ruzek KA,Wenger DE. The multiple faces of lymphoma of the musculoskeletal system. Skeletal Radiol. 2004;33:1-8.
- Masaoka S, Fu T. Malignant lymphoma in skeletal muscle with rhabdomyolysis: a report of two cases. J Orthop Sci. 2002;7:688-93.
- McClement JMF, Webb IN. Tumors arising in skeletal muscle in adults. J Pathol. 1976;118:112-20.
- Chim CS, et al. Primary skeletal muscle lymphoma. Am J Med. 2002;112:79-80.
- Marotta D, et al. Soft tissue non-Hodgkin lymphoma of the shoulder in an HIV patient: a report of a case and review of the literature. World J Surg Onco. 2008;6:111.
- Takagi A, et al. Rippling muscle syndrome preceding malignant lymphoma. Internal Medicine 2002;41:147-50.
- Hosono M, et al. Involvement of muscle by malignant lymphoma: MR and CT appearances.J Comput Assist Tomogr. 1995;19:455?9.
- Malloy PC, Fishman EK, Magid D. Lymphoma of bone, muscle, and skin: CT findings. AJR Am J Roentgenol. 1992;159:805?9.
- Lee VS, MartinezS, Coleman RE. Primary muscle lymphoma: clinical and imaging findings. Radiology. 1997;203:237-44.
|