Abstract
Abdominal injury with a metallic object is a rare condition when war zones are excluded. The foreign body penetrates the body by forming an open wound, and the damage depends on the density of the adjacent organs, the character of the metallic object and the energy of the trauma.
In our article; we evaluated the management of a 72-year-old male patient with hypertension, who allegedly injured the suprapubic region with an anchor while engaged in agriculture about an hour before his admission to the emergency room. Hemodynamically stable patient was resuscitated according to the current Emergency Management of Severe Trauma (EMST) guidelines, emergency laparotomy was decided after major vascular injury was excluded by angiography. Result : The V-shaped metallic foreign body was approximately 1 meter long, 3 kg, 5 cm wide and 2 cm thick. By making an incision extending from the entrance of the foreign body to the umbilicus and providing adequate vision; The body was removed under the control of bleeding. There was no major vascular injury in the examination, and the defect in the sigmoid colon meso was repaired ;orthopedic physicians applied debridement for the crack in the pubic tubercle. The patient who received ceftiriaxone, metronidzol, gentamicin antibiotics; He was discharged uneventfully on the 17th postoperative day after the purulent flux from incision was controlled.
Angiography is useful in excluding great vessel injury in hemodynamically stable patients with impalement injury and the process requires a multidisciplinary approach.
Keywords :
Implament Injury
, Penetrant trauma
, Angiograpy
Turkish Abstract
Metal bir cisimle karın yaralanması, savaş bölgeleri hariç tutulduğunda nadir görülen bir durumdur.
Yabancı cisim açık bir yara oluşturarak vücuda girer ve hasar komşu organların yoğunluğuna, metalik cismin karakterine ve travmanın enerjisine bağlıdır.
Yazımızda; acil servise başvurmadan yaklaşık bir saat önce tarımla uğraşırken suprapubik bölgeyi çapa ile yaraladığı iddia edilen 72 yaşında hipertansiyon tanılı erkek hastanın yönetimini değerlendirdik.
Hemodinamik olarak stabil olan hasta, mevcut Şiddetli Travma Acil Durum Yönetimi (EMST) kılavuzlarına göre resüsite edildi, majör vasküler yaralanma anjiyografi ile ekarte edildikten sonra acil laparotomiye karar verildi.
V şeklindeki metalik yabancı cisim yaklaşık 1 metre uzunluğunda, 3 kg, 5 cm genişliğinde ve 2 cm kalınlığındaydı. Yabancı cismin girişinden göbek deliğine kadar uzanan ve yeterli görüş sağlayan bir kesi yapılarak; metalik cisim kanama kontrolü altında çıkarıldı.
Eksplorasyonda majör damar yaralanması yoktu ve sigmoid kolon mezosundaki defekt onarıldı, ortopedi kliniğince pubik tüberküldeki çatlak için debridman uyguladı. Seftiriakson, metronidzol, gentamisin antibiyotikleri alan hasta; insizyondan pürülan akıntı kontrol altına alındıktan sonra postoperatif 17. günde sorunsuz taburcu edildi.
Anjiyografi, hemodinamik olarak stabil ve penetran yaralanması olan hastalarda büyük damar yaralanmasını dışlamada faydalıdır ve süreç multidisipliner bir yaklaşım gerektirir.
Turkish Keywords :
, İmpalante Yaralanma
, Penetran Travma
, Anjiyografi
Introduction
Injury with a metallic foreign body creates an open wound and penetrates the body; It causes damage to the body according to the density of nearby organs, the characteristics of the object and the energy of the trauma 1. Excluding battle fields, metallic foreign body injury - impalement injury is a rare form of penetrating injury 2-3.
Abdominal foreign body injury is also often associated with major vessel injury and requires a multidisciplinary approach before hospital, transporting, during and after surgery 4.
In our article; we evaluated the management of a 75-year-old male patient with hypertension, who allegedly injured the suprapubic region with an anchor while engaged in agriculture about an hour before his admission to the emergency room.
Case Report
A 72-year-old male patient with a diagnosis of hypertension was reportedly injured in the suprapubic region while working in agriculture approximately one hour before being brought to the emergency room. In the emergency department evaluation, he was conscious and cooperative (E4, M6, V5), and his blood pressure was 110/70 mm Hg; his heart rate was 90 beats per minute; peripheral pulses could be taken, and the left lower quadrant of his abdomen was tender. Foreign body entry site from the left suprapubic region; anterior surface of the right tibia had a subcutaneous skin laceration. There are no motor deficits in the patient's extremities. The calculated Injury Severity Score was 36.
The patient with stable hemodynamics received resuscitation in accordance with the Emergency Management of Severe Trauma (EMST) guidelines. Antibiotics with a broad spectrum and tetanus prophylaxis were administered. Utilizing Focused Abdominal Sonography, a urinary catheter was inserted. There was no evidence of hematuria in the urine, and minimal free fluid was detected in the pelvis.
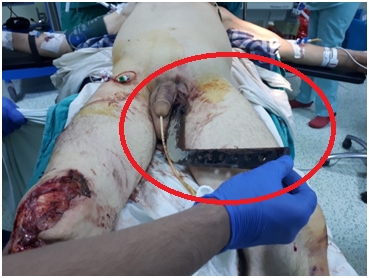
Angiography was performed to detect femoral artery and vein injury due to the anatomical proximity and patient's stability. The angiography performed by the vascular surgery team did not account for bleeding in the left femoral artery, vein, or branches. Afterward, we consulted with the patient. As a result of the evaluation, the patient's pubic bone and pelvis were evaluated by orthopedic physicians using a radiography image (Figure 4) prior to surgery, and the decision was made to perform an emergency laparotomy to detect damage and remove the foreign object (Figure 1).
The V-shaped metallic foreign body measured approximately 1 meter in length, 3 kilograms in mass, 5 centimeters in width, and 2 centimeters in thickness. By making an incision extending from the foreign body's entrance to the umbilicus and ensuring adequate visibility (Figure 2 -3), the body was extracted while the bleeding was controlled. The examination revealed no major vascular and solid organ injuries, and the defect in the sigmoid colon meso was repaired without disrupting colon blood supply. Orthopedic physicians performed debridement on the pubic tubercle fracture. The anterior portion of the right tibia that had been laser-treated was repaired.
Following the placement of a drain in the abdomen, the operation was concluded. After one day of intensive care unit follow-up, the patient was followed by the continuation service. During hospitalization, ceftrikason 2.1 grams, metronidazole 3.500 milligrams, and gentamicin 1.160 milligrams were administered. After controlling the purulent discharge from the incision, he was discharged from the hospital on the 17th day without incident.
Discussion
It is stated that penetrating injuries are uncommon, but they account for 15% of trauma-related deaths when battlefields are excluded. [2,3,5] The foreign object enters the body through an open wound, and the severity of the damage depends on the density of the adjacent organs, the nature of the metallic object, and the force of the trauma. 1
According to the mechanism of injury, there are three distinct types of implant injuries. Class 1: striking a fixed object, such as when falling from a height; class 2: penetrating a moving object; class 3: combination of classes 1 and 2. 4 Our case report describes a type 2 penetrating injury.
It is advised not to manipulate the foreign body in order to prevent additional bleeding, as this may eliminate the tamponade effect. However, the object can be shortened in order to properly position the patient for surgery. To prevent further damage to the body, it is crucial that the patient remains as stable as possible and arrives at the trauma center as soon as possible for optimal results. 4 According to reports, our patient arrived at the hospital within an hour, and there was no need to shorten the foreign body.
The patient should be administered broad-spectrum antibiotics and tetanus prophylaxis because the foreign body is highly contaminated. 4 Depending on the characteristics of the foreign body and the direction of entry, it is necessary to identify potentially damaged structures and plan treatment. At this point, a multidisciplinary team is required to treat a multisystem injury. Hemodynamic stability cannot rule out vascular damage. 4
Vascular injuries are highly likely to accompany abdominal implant injuries. 4 When there is no external source of bleeding, it is challenging to detect vascular damage, particularly in the lower extremities. By using physical examination, vascular damage can be identified and surgery indicated. In order to determine when to intervene in vascular injury, symptoms and signs can be categorized as hard or soft signs. The hard sign indicates arterial bleeding, pulselessness, a hematoma that is expanding, and ischemia. A soft sign is the presence of a history of prehospital blood loss, decreased pulse, proximity to major vessels, and ipsilateral neurologic deficit. Classic symptoms, including paresthesia, pulsationlessness, paralysis, pain, bruising, and coldness, can also detect vascular damage to the lower extremities. A rigid sign indicates the need for immediate surgery. Nonetheless, negative clinical findings cannot rule out vascular damage.6 In our patient's case, only one soft sign was present, and it was close to the major vascular structure.
The gold standard for detecting the location and extent of vascular damage with high sensitivity and low morbidity is angiography. As a complementary diagnostic technique, it is extremely useful for detecting vascular damage in the emergency room. However, it is invasive and requires a specialized team and equipments. [6] We performed angiography to detect potential vascular damage in a patient who was stable, lacked a hard sign, and did not require emergency vascular intervention. The patient with undetected vascular damage was transferred to us. Examining the case reports and reviews of abdominal implant injury in the medical literature reveals that angiography was never used.1,7,4,8,9,10
Catheter-based angiography is the gold standard for the diagnosis of peripheral vascular trauma; however, it has been largely replaced by Computed Tomography Angiograpy (CTA) over the past decade due to the simple integration of extremity CTA with torso imaging in trauma patients and the improved image quality brought about by advancements in CT technology. CTA has the advantages of being less traumatic, more widely available, and permitting the assessment of nearby soft tissues and bones .CTA minimizes the possible preventable complications of catheter angiography, including pseudoaneurysm, hemorrhage, thrombosis of the access vessel, and peripheral embolization .11
Incision in laparotomy should be performed so as to guarantee the removal of the foreign body through direct inspection and control of bleeding. Upon completion of the exploration, the foreign body should be extracted under control of bleeding using direct examination. 4
20-80% of penetrating injuries cause peritoneal disruption. In trauma patients, injuries to hollow organs are associated with morbidity and mortality, despite not being the source of hemodynamic stability. According to damage control surgery practice, the timing and technique of hollow organ repair in hemodynamically unstable patients should be emphasized 7. Since our patient was hemodynamically stable, we were able to repair the colon meso without interfering with the colon's blood supply.
Appropriate lavage and debridement are required from the entry site of the foreign body to its trace. A drain can be placed when necessary.4
Informed Consent
From the patient
References
- Mittal, Chaitanya et al. “Fatal penetrating abdominal injury by a metallic projectile.” Journal of forensic sciences, 10.1111/1556-4029.14828. 2 Aug. 2021, doi:10.1111/1556-4029.14828
- Störmann, P et al. “Epidemiology and outcome of penetrating injuries in a Western European urban region.” European journal of trauma and emergency surgery : official publication of the European Trauma Society vol. 42,6 (2016): 663-669. doi:10.1007/s00068-016-0630-4
- Katiyar, Awaneesh et al. “An unusual mechanism of hook impalement injury - A case report.” Trauma case reports vol. 28 100332. 30 Jun. 2020, doi:10.1016/j.tcr.2020.100332
- Mohan, Rajashekar et al. “Transabdominal impalement: absence of visceral or vascular injury a rare possibility.” The Journal of emergency medicine vol. 41,5 (2011): 495-8. doi:10.1016/j.jemermed.2008.03.033
- Søreide, K. “Epidemiology of major trauma.” The British journal of surgery vol. 96,7 (2009): 697-8. doi:10.1002/bjs.6643
- Liu, Jian-Long et al. “Literature review of peripheral vascular trauma: Is the era of intervention coming?.” Chinese journal of traumatology = Zhonghua chuang shang za zhi vol. 23,1 (2020): 5-9. doi:10.1016/j.cjtee.2019.11.003
- Papanikolas, Michael J et al. “Suprapubic penetrating abdominal trauma - defining peritoneal breach and choices in operative intervention.” Journal of surgical case reports vol. 2019,11 rjz336. 20 Nov. 2019, doi:10.1093/jscr/rjz336
- Ugoletti, Lara et al. “Gluteal, abdominal, and thoracic multiple impalement injuries: A case report on management of a complex polytrauma.” Medicine vol. 98,22 (2019): e15824. doi:10.1097/MD.0000000000015824
- Ozaydin, Seyithan et al. “Penetrating injury caused by a long iron bar: A case report.” Northern clinics of Istanbul vol. 5,1 75-78. 11 Jan. 2018, doi:10.14744/nci.2017.75508
- Sankpal, Jitendra et al. “Thoraco-abdominal impalement injury with two construction iron bars - A rare case report.” International journal of surgery case reports vol. 67 (2020): 80-81. doi:10.1016/j.ijscr.2020.01.0304
- Walkoff, Lara et al. “Imaging primer for CT angiography in peripheral vascular trauma.” Emergency radiology vol. 28,1 (2021): 143-152.
|