Abstract
Gastric volvulus is a rare cause of acute abdominal pain. It can be easily diagnosed with the development of radiologic imaging modalities and the diagnosis should not be missed. Volvulus can be idiopathic or secondary due to diseases. Ischemia and necrosis rarely occur due to the rich blood supply of the stomach. Herein, we presented a case of gastric volvulus underlying pyloric stenosis with chronic gastric dilatation and we aimed to discuss the treatment options.
Keywords :
volvulus
, stomach
, acute abdomen
Turkish Abstract
Gastrik volvulus, akut karın ağrısının nadir bir nedenidir. Radyolojik görüntüleme yöntemlerinin gelişimi ile kolayca teşhis edilebildiği için tanı kaçırılmamalıdır. Volvulus idiopatik veya çeşitli hastalıklara sekonder olabilir. İskemi ve nekroz, midenin zengin kan dolaşımı nedeniyle nadiren oluşur. Burada, kronik gastrik dilatasyon ile birlikte pilor stenozuna bağlı bir gastrik volvulus olgusu sunmayı ve tedavi seçeneklerini tartışmayı amaçladık.
Turkish Keywords :
, volvulus
, mide
, akut karın
Introduction
Gastric volvulus is a rare and life-threatening condition. It can be seen at all ages, predominantly in adults after the 5th decade of life. Thirty percent of cases are idiopathic, while 70% are secondary to paraesophageal hernia, diaphragmatic eventration, diaphragmatic paralysis, adhesions, neoplasm, or trauma. About one-third of reported cases present with acute onset, meanwhile the others have more chronic or intermittent symptoms 1.
Gastric volvulus has no specific clinical or laboratory findings, and the diagnosis is usually established intraoperatively. Preoperative radiologic diagnosis of gastric volvulus is also difficult and important. Especially, computed tomography (CT) is important in early diagnosis in order to allow immediate surgical intervention and to prevent life-threatening complications 2,3.
Case Report
A thirty-one year old female patient admitted to our emergency department with an abdominal pain. She had a history of episodic abdominal pain for the last 9 months with abdominal distention, nausea and vomiting. She had a hard vaginal birth history 11 months ago and her symptoms started following delivery and symptoms were activated while eating. She has been taking gastroprotective medication for 15 years.
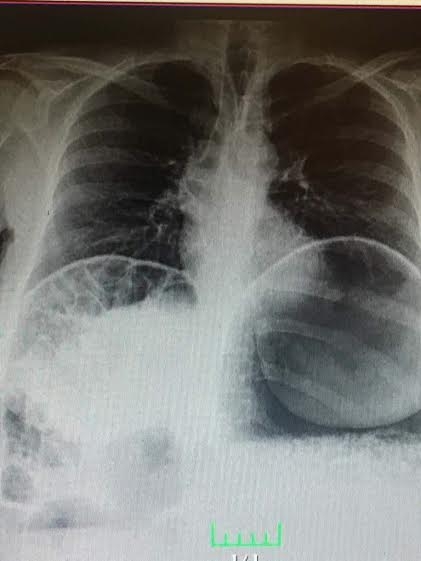
The serum potassium level was 3.31 mEq/L (3.5-5.5) and amilase level was 171 mg/dL (28-100). Other laboratory tests were within normal limits. There was not any free air under the diaphragm on chest X-ray and there were not any chest diseases. On plain abdominal graphy, a large gas distention in the gastric fundus was (Figure 1).
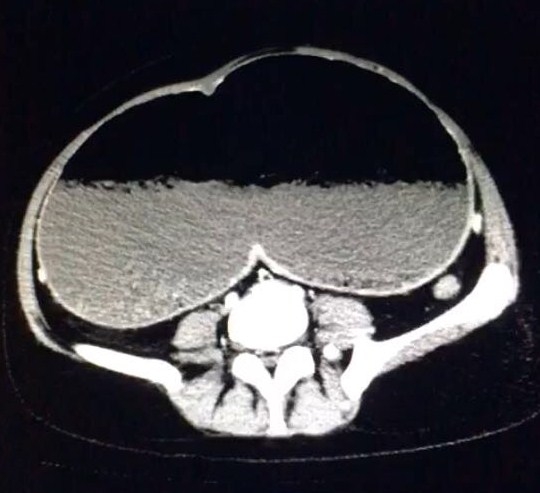
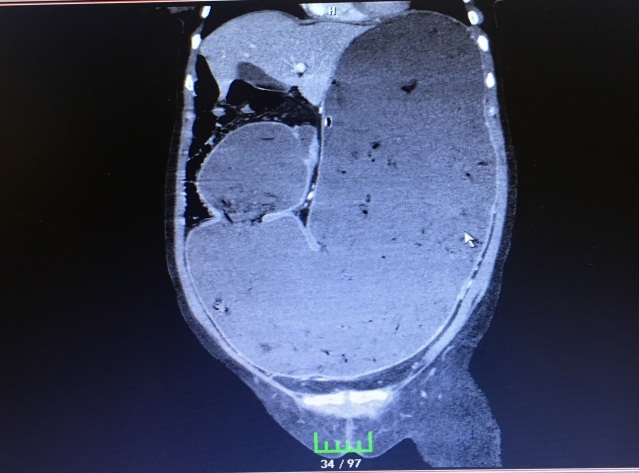
On contrast enhanced abdominal CT, a narrowed segment in the pylori and large distention of the stomach were observed (Figures 2-3).
Gastric volvulus on the CT scans was detected. Gastric decompression was performed by nasogastric catheter and approximately 2000cc gastric content was drained. Balanced electrolyte solution and hydration was administered. After that, upper gastrointestinal endoscopy was performed.
The antrum and pylori could not be visible by gastrointestinal endoscopy. Gastric decompression and detorsion of the stomach was successfully performed endoscopically. After the decompression, the symptoms of the patient resolved immediately. On the 3rd day of the detorsion, control upper gastrointestinal endoscopy was performed. Deformation of the bulbus and post bulbar stenosis were observed endoscopically. An elective surgery for post bulbar stenosis was planned and the patient was discharged from the hospital.
Discussion
The incidence of stomach volvulus is equal among all races and genders 1. The cases without accompanying other abdominal pathologies or diseases and those occur due to the massive elongation of the gastric bundles are called as ?idiopathic volvulus?. In three quarter of cases, it may appear secondary to other pathologies. These pathologies include eventration of the left hemi diaphragm, hiatal hernia, intraabdominal cohesions and pyloric stenosis 2.
It can be classified into 4 groups due to the mechanism of development 3.
Type 1 (Organoaxial): It occurs by the rotation of the stomach along its long axis (along the cardio pyloric line, which is drawn between the cardia and the pylorus). It represents 59% of all cases.
Type 2 (Mesenteroaxial): It occurs by rotation of stomach around short axis from the lesser to greater curvature (i.e. perpendicular to the cardiopyloric line). It counts 29% of the cases.
Type 3 (combined form): it represents 2% of all cases.
Type 4 (unclassified form): It counts 10% of the cases.
Borchardt?s triad (unproductive retching, epigastric pain and unsuccessful passage of nasogastric tube into the stomach) can be used as diagnostic criteria of gastric volvulus 4. However, the classic triad occurs in only three quarters of cases. Upper gastrointestinal barium studies and abdominal CT are helpful radiologic imaging methods.
Gastric volvulus rarely causes acute abdomen. The rich vascular supply of the stomach prevents the stomach and gangrene of the stomach is a rare condition. The most common type causing acute abdomen is organoaxial type of volvulus. Chronic gastric volvulus is more common than the acute form and it can be symptomatic or asymptomatic. Asymptomatic gastric volvulus cases can be incidentally diagnosed by radiologic examinations. In symptomatic cases upper abdominal distention, tenderness, persistent or colic pain may occur and the symptoms are generally mild. While eating, distention and tenderness, retching and vomiting may occur.
Progressive distention and nonproductive retching may follow the pain 2. In our case there was a chronic symptomatic volvulus.
Detorsion of the gastric volvulus can be treated successfully by open or laparoscopic methods. If the stomach is strangulated or necrotic, gastric resection may be required 3. In our case, endoscopic detorsion and decompression was successfully performed. The patient was fine on the 5th month of the gastric decompression.
References
- Chau B, Dufel S. Gastric volvulus. Emerg Med J. 2007;24:446-7. doi:10.1136/ emj.2006.041947
- Ellis H. (çev: Andican A.) . Divertikül volvulus ve ileus. In: Schwartz SI, Ellis H., ed(s) (çev editörü: Andican A.). Maingot Abdominal Operasyonlar. 8. baskı. İstanbul: Nobel Tıp Kitabevi; 1989: 531-48.
- Lee TC, Liu KL, Lin MT, Wang HP. Unusual cause of emesis in an octogenarian: organoaxial gastric volvulus associated with paraesophageal diaphragmatic hernia. J Am Geriatr Soc. 2006; 54:555-7.
- Germanos S, et al. Severe abdominal pain as a result of acute gastric volvulus. Int J Emerg Med. 2010; 3:61-2. doi:10.1007/ s12245-009-0136-5
|