Abstract
Burkitt lymphoma is the most common subtype of non-Hodgkin's lymphoma in childhood. Although, Burkitt lymphoma mostly involves the head and neck in children, the gastrointestinal tract, genitourinary tract, gonads, mesentery, peritoneum, and retroperitoneum are also potential sites of involvement. Herein, we report computed tomography (CT) findings of hepatic, pancreatic, kidney, and peritoneal involvement of intestinal Burkitt lymphoma in a pediatric case.
Keywords :
Burkitt lymphoma
, Computed tomography
, Pancreatic involvement
Turkish Abstract
Burkitt lenfoma, çocukluk çağı non-Hodgkin lenfomaların en sık görülen alt tipidir. Çocuklarda en sık olarak baş ve boyunu tutmasıyla beraber, gastrointestinal yapılar, genitoüriner sistem, gonadlar, mezenter, periton ile retroperitoneal bölgeler de potansiyel tutulum alanlarıdır. Bu yazımızda , pediatrik intestinal Burkitt lenfoma olgusunun hepatik, pankreatik, böbrek ve peritoneal tutulumunun bilgisayarlı tomografi bulgularını sunuyoruz.
Turkish Keywords :
, Burkitt lenfoma
, Bilgisayarlı tomografi
, Pankreatik tutulum
Introduction
Burkitt lymphoma is the most common subtype of non-Hodgkin's lymphoma in childhood and reported for approximately 34% of these cases. It is the most rapidly growing tumor in children with a doubling time of approximately 24 hours 1,2.
There are various abdominal and pelvic imaging findings in Burkitt lymphoma affecting solid organs and the gastrointestinal tract. Burkitt lymphoma mostly involves the head and neck, gastrointestinal tract, genitourinary tract, gonads, mesentery, peritoneum, and retroperitoneum 3. Recognition of the imaging findings is critical in the consideration of Burkitt lymphoma as a potential diagnosis to initiate therapy early in patients, as prompt supportive care and therapy are essential 3.
Herein, we report computed tomography (CT) findings of hepatic, pancreatic, kidney, and peritoneal involvement of intestinal Burkitt lymphoma in a pediatric case.
Case Report
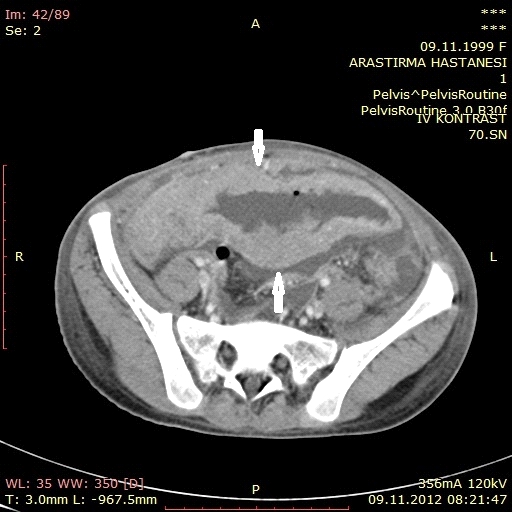
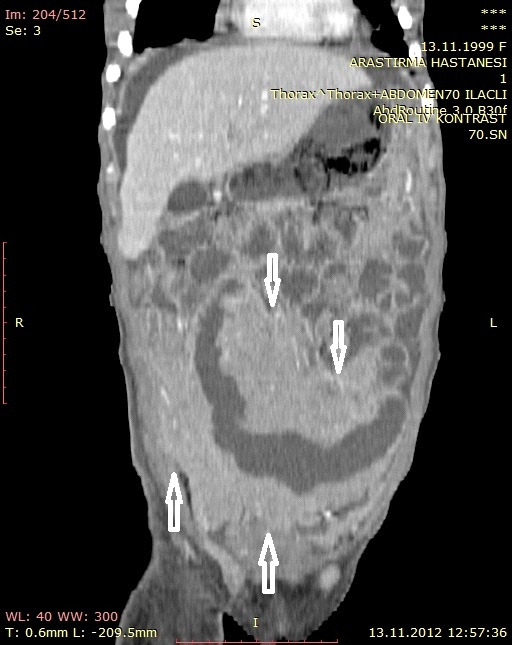
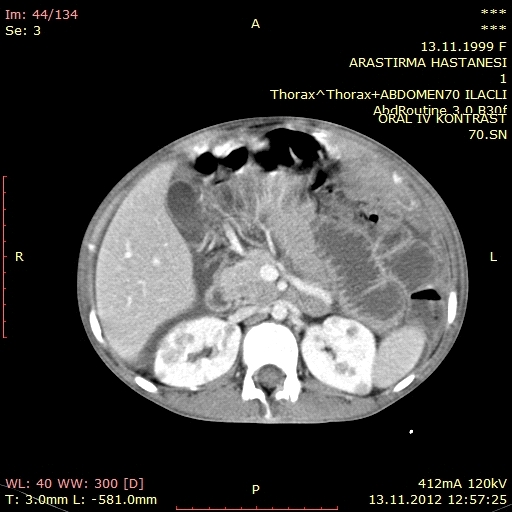
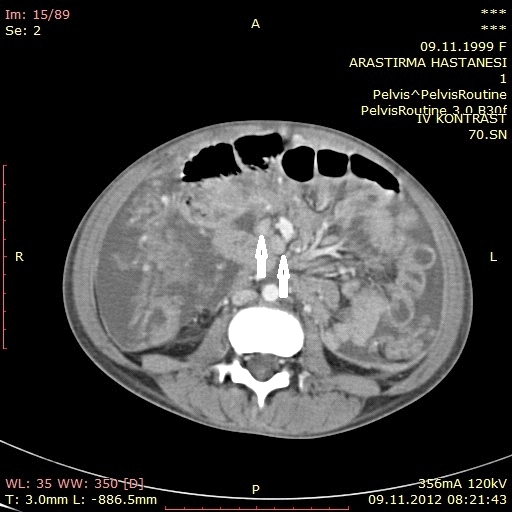
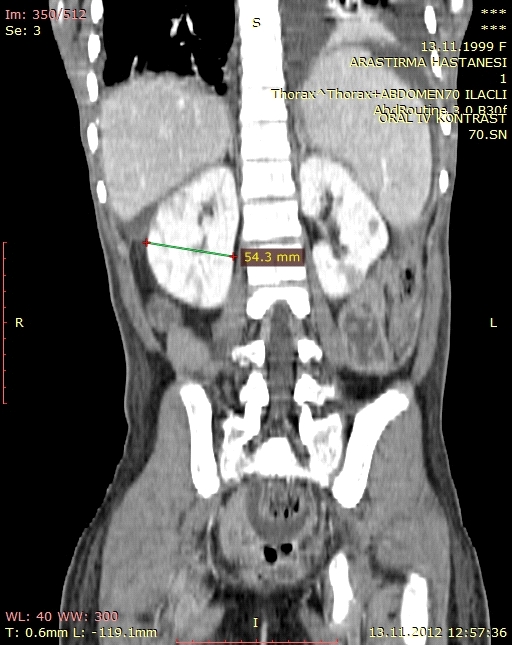
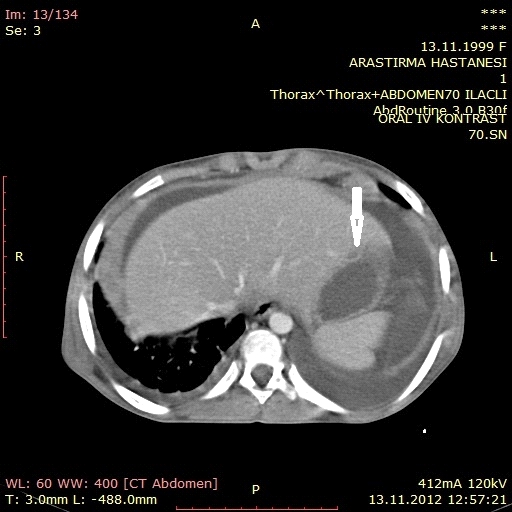
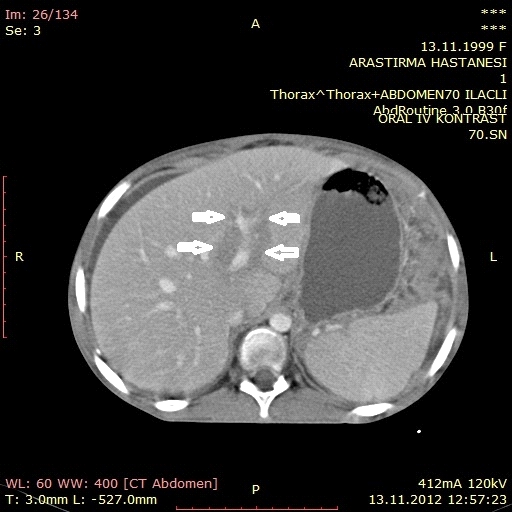
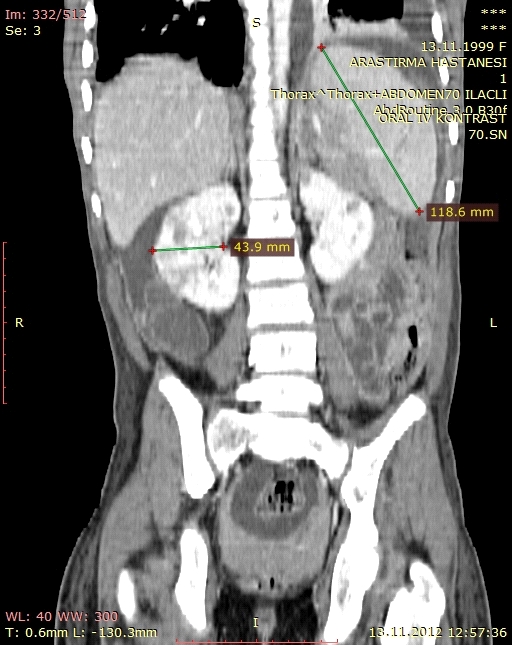
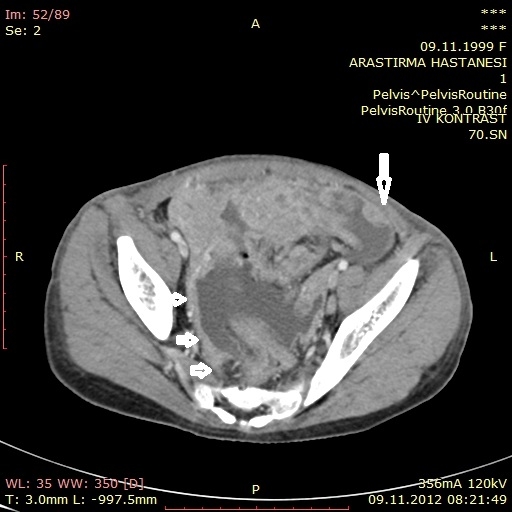
A 13-year-old girl was admitted to pediatric emergency clinic with severe nausea and vomiting for two days and abdominal swelling and pain for three days. Her medical history was unremarkable. Physical examination revealed hepatosplenomegaly and a mass aligning from umbilicus to the right lower quadrant. On abdominal ultrasonography (USG), mild hepatosplenomegaly and pancreatic diffuse hypoechogenous mass lesions, the largest being 21x20 mm in size, were demonstrated. A 23x6 cm heterogenous, well-vascularized hypoechoic mass lesion was extending from the right periumbilical region to the right lower quadrant with multiple adjacent lymph nodes. A contrast enhanced abdominal CT examination showed a 25x7x6-cm ileal mass, originating from the wall of proximal ileum and extending to the right lower quadrant and multiple adjacent retroperitoneal and left inguinal pathological lymph nodes. In addition, diffuse pancreatic enlargement and mild renal enlargement with multiple hypodense lesions were noted. A small similar hypodense lesion in the liver and a periportal infiltrative mass were detected. Ascites, peritoneal thickening and nodules consisting of seeding metastasis and left-sided pleural effusion were also shown (Figures 1,2,3,4,5,6,7,8,9,10,11,12).
All these radiological findings were suggestive of a malignant metastatic ileal tumor. Pathological examination of the lymph node biopsy samples revealed high-grade, non-Hodgkin, B-cell lymphoma. Immunohistochemical testing was also positive for CD45, CD20, CD10, and BCL-6, and negative for CD3, TdT, and BCL-2, which was consistent with Burkitt's lymphoma. The patient who was treated with combined chemotherapy responded well to the treatment.
Discussion
Burkitt lymphoma was first described in 1958 in Uganda by a surgeon who observed rapidly enlarging tumors in children involving the jaw 3. It is classified by the World Health Organization into three types: endemic, sporadic, and immunodeficiency-associated types 3. The endemic form is found mostly in equatorial Africa and Papua New Guinea, and is associated with the Epstein-Barr virus in the majority of cases 3. The sporadic (or American) form is found in the North America, Northern and Eastern Europe, and Far East, and is associated with the Epstein-Barr virus in 15% of patients 4. Although, Burkitt lymphoma mostly involves the head and neck in children, the gastrointestinal tract, genitourinary tract, gonads, mesentery, peritoneum, and retroperitoneum are also potential sites of involvement 3, 5. Intrinsic involvement within the gastrointestinal tract has been reported to occur in 22.5% of cases, abdominal or pelvic masses in 45% of cases, and hepatic lesions in 17% of cases, with the predominance of these cases occurring in children 5.
The diagnostic work-up for Burkitt lymphoma, as in any other form of non-Hodgkin's lymphoma, is definitive by tissue diagnosis 3 . Cross-sectional imaging is necessary to identify the distribution, severity, and staging to implement appropriate therapy. Imaging techniques most often used include USG, CT, positron-emission tomography (PET)/CT, gallium scintigraphy, and bone scintigraphy. Initially, USG is used, if a child presents with an abdominal or pelvic mass. In addition, CT often follows USG to provide a more global assessment for bowel and visceral involvement, as well as the tumor staging. Due to the concerns relating to radiation risk for oncology patients, particularly pediatric patients, with repeated imaging studies, magnetic resonance imaging (MRI) has gained importance in recent years 3.
The terminal ileum is the most commonly reported location of Burkitt lymphoma in children, likely due to the high concentration of lymph tissues in that region of the bowel 5. Imaging findings on CT include a focal mass and diffuse thickening of the bowel wall 1.
Hepatic involvement in Burkitt lymphoma is approximately 17% 3. The most common findings on CT are discrete areas of low attenuation which may be solitary or multi-centric. A periportal infiltrating mass, which is low in attenuation on CT and hypoechoic on USG, has also been reported with or without distal biliary duct dilatation 6.In our case a periportal infiltrating mass and a solitary lesion were also demonstrated.
Although, spleen involvement is uncommon in Burkitt lymphoma, the most common radiological finding is diffuse splenomegaly. Other radiological findings include hypoechoic splenic lesions on USG and low-attenuation lesions on CT examination 5.Diffuse splenomegali was shown in our patient.However, we did not demonstrate any focal splenic lesion.
Furthermore, CT findings of renal involvement of Burkitt lymphoma most commonly include nephromegaly in 90% of cases 3. Focal renal masses (30%) and hydronephrosis due to ureteral obstruction (50%) are also seen. On USG, kidneys may show an increased cortical echogenicity (60%) with or without iso- or hypoechoic masses. Renal calculi associated with tumor lysis syndrome after chemotherapy have been also reported on USG and CT 7.Bilateral renal masses and bilateral nephromegaly were seen in our patient but imaging studies did not show hydronephrosis or renal calculi.
Pancreas is involved in Burkitt lymphoma in approximately 10% of cases 3. Computed tomography findings include focal pancreatic enlargement with patchy areas of non-enhancement. Marked dilatation of the biliary system can also occur, when a mass infiltrates the pancreatic head 3.In our patient pancreatic enlargement with multipl focal lesions was evident .Although there was no dilatation of the biliary system.
The involvement of the lymph nodes in the mesentery and retroperitoneum by Burkitt lymphoma frequently presents as abdominal and pelvic masses. These masses may be large and single or multiple in the abdomen or pelvis, while some may have necrotic centers containing fluid 3.
Ascites is a common finding which occurs in 25% of patients with Burkitt lymphoma 6. The diagnosis of Burkitt lymphoma is often made by evaluation of paracentesis 1. Although, lymphomatous involvement of the peritoneum is uncommon in children, it is usually associated with marked bowel or mesenteric inflammation. In addition, CT findings of Burkitt lymphoma can mimic mucinous tumors in adults and, therefore, can be misdiagnosed as desmoplastic small-round-cell tumors in children and adolescents, which may have a similar clinical presentation 8. The findings on CT include nodularity along the peritoneal reflections and hepatic capsule with peritoneal ascites. On USG, peritoneal involvement is seen as hypoechoic mesenteric masses or, rarely in Burkitt lymphoma, as omental cakes 3,9,10.We demonstrated mesenteric nodüles,omental cakes and marked ascites in our patient.
In conclusion, the imaging findings in Burkitt lymphoma are variable, and it may involve multiple organs and tissues. Therefore, a thorough evaluation of the whole abdomen is critical for early diagnosis and treatment.
References
- Hamrick-Turner JE, et al. Imaging of childhood non-Hodgkin lymphoma: assessment by histologic subtype. RadioGraphics. 1994; 14:11-28.
- Eren S, Kantarci M, Erdogan F. Ovarian Burkitt's lymphoma as a cause of ?omental cake? sign on computerised tomography. J Obstet Gynaecol. 2004; 24:463-5.
- Biko DM, Anupindi SA, Hernandez A, Kersun L, Bellah R. Childhood Burkitt lymphoma: abdominal and pelvic imaging findings. AJR Am J Roentgenol. 2009;192(5): 1304?15.
- Ferry JA. Burkitt's lymphoma: clinicopathologic features and differential diagnosis. Oncologist. 2006; 11:375-83.
- Dunnick NR, et al. Radiographic manifestations of Burkitt's lymphoma in American patients. AJR. 1979; 132:1-6.
- Krudy AG, et al. CT of American Burkitt lymphoma. AJR. 1981; 136:747-54.
- Strauss S, et al. Renal sonography in American Burkitt lymphoma. AJR. 1986; 146:549-52.
- Bellah R, et al. Desmoplastic small round cell tumor in the abdomen and pelvis: report of CT findings in 11 affected children and young adults. AJR. 2005; 184:1910-4.
- Toma P, Granata C, Rossi A, Garaventa A. Multimodality imaging of Hodgkin disease and non-Hodgkin lymphomas in children. RadioGraphics. 2007; 27:1335-54.
- Goodman P, Raval B. Omental cakes in American Burkitt lymphoma: computed tomography demonstration. Clin Imaging. 1989; 13:117-8.
Information Presentation
Turkrad Radyoloji Kongresi 2016 :Poster sunumu(Türkçe)
|