Abstract
Gastric volvulus is a rare but life-threatening cause of upper gastrointestinal obstruction. About one-third of reported cases occur with acute onset and there is no specific laboratory or clinical findings. It can cause serious complications like gastric ischemia, necrosis or perforation; if occurs, rapid recognition and prompt surgical intervention are required. Mesenteroaxial form contains 29% of all cases and results in gastric ischemia more than other types. Here, we present a 46 year-old female patient with acute mesenteroaxial gastric volvulus. If gastric volvulus is one of the differential diagnoses, imaging studies become important. Computed tomography (CT) should be preferred as the first method of imaging for prompt diagnosis and surgical intervention because it enables multiplanar demonstration as well as providing valuable information about possible etiologies, complications and predisposing factors.
Keywords :
Acute abdomen
, Gastric
, Mesenteroaxial volvulus
Turkish Abstract
Gastrik volvulus, üst gastrointestinal sistem obstrüksiyonunun nadir bir nedenidir. Vakaların yaklaşık üçte biri akut başlangıçlı olup tanıya spesifik bir laboratuvar bulgusu ya da klinik bulgu mevcut değildir. Gastrik iskemi, nekroz ya da perforasyon gibi ciddi komplikasyonlara sebebiyet verebileceğinden gastrik volvulus oluşması halinde hızlı tanı ve acil cerrahi müdahale gereklidir. Mezenteroaksiyel form vakaların % 29?unu oluşturmaktadır. Diğer alt tiplere göre mezenteroaksiyel volvulusta gastrik iskemi daha sık gelişir. Eğer gastrik volvulus akla gelen bir ön tanı ise görüntüleme yöntemleri önem arz etmektedir. Multiplanar görüntüleme imkanı sağlaması; komplikasyonlar, etiyolojik sebepler ya da predispozan faktörler hakkında kıymetli bilgiler vermesi açılarından bilgisayarlı tomografi (BT) hızlı tanı ve acil cerrahi girişim için ilk tercih edilmesi gereken görüntüleme metodu olmalıdır.
Turkish Keywords :
, Akut abdomen
, Gastrik
, Mezenteroaksiyel volvulus
Introduction
Gastric volvulus is a rare and life-threatening condition. It can be seen at all ages, predominantly in adults after the 5th decade of life. Thirty percent of cases are idiopathic, while 70% are secondary to paraesophageal hernia, diaphragmatic eventration, diaphragmatic paralysis, adhesions, neoplasm, or trauma. About one-third of reported cases present with acute onset, meanwhile the others have more chronic or intermittent symptoms 1.
Gastric volvulus has no specific clinical or laboratory findings, and the diagnosis is usually established intraoperatively. Preoperative radiologic diagnosis of gastric volvulus is also difficult and important. Especially, CT is important in early diagnosis in order to allow immediate surgical intervention and to prevent life-threatening complications 2,3.
Case Report
A 46 year-old female patient presented to the emergency department with acute onset of epigastric pain and nausea. She had no other gastro-intestinal tract symptom.
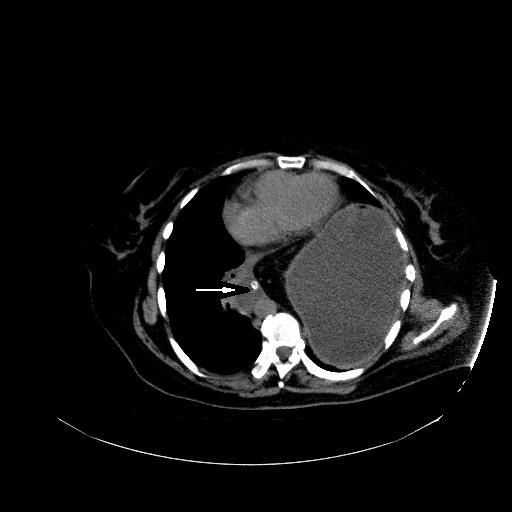
She did not have any chronic medication, history of abdominal surgery or trauma. She was referred to emergency radiology clinic and abdominal sonography was performed. Stomach was seen obviously distended. Clinicians attempted to use a nasogastric tube to decompress the stomach. Seeing that the tube cannot be placed; the suspicion of a gastric volvulus came to mind. CT of the abdomen was requested. No IV contrast was administered because creatinine level of patient is too high ( 4 mg/dl). Oral contrast administration also could not be tolerated by the patient. CT demonstrated a high-positioned stomach without normal gastric axis and appearance (Figure 1, 2). The stomach had an abnormal transverse orientation. Distal corpus, antrum and pylorus were located superiorly with respect to fundus (Figure 3). And also a hiatal defect was present and stomach was herniated into the thorax via the defect (Figure 4) (type 3-mixed type hiatal hernia). Radiologically mesenteroaxial gastric volvulus was present. The patient was taken for emergency surgery soon thereafter. The diagnosis of mesenteroaxial gastric volvulus was confirmed intraoperatively.
In surgery, the omentum was replaced into the abdomen, the stomach was detorsioned, and the diaphragmatic defect was repaired. After 2 days from the surgery clinical and laboratory findings returned to normal, and oral intake was allowed. The patient was discharged 6 days after the surgery.
Discussion
Gastric volvulus is defined as an abnormal rotation of the stomach along its one or both axis more than 180 degrees, causing a closed loop obstruction. Acute gastric volvulus is less common and a life-threatening surgical emergency. It can result in important complications like gastric ischemia, necrosis or perforation; seeing that rapid recognition and prompt surgical intervention is required 4. Mortality rates may be as high as 30?50% 5.
Gastric volvulus can be classified based on axis of rotation, onset (acute or chronic), extent (total or partial) or etiology (primary or idiopathic)]. Most frequently gastric volvulus classified into four subgroups. Type 1, most common type (59%), (organoaxial form) results from rotation of the stomach around the pylorus?cardia axis. It may cause obstruction in the gastro esophageal junction, pylorus, or both. Type 2 (mesenteroaxial form), accounting for 29% of all cases, occurs as a result of a rotation around the lesser?greater curvature axis. Type 3 (combined form), accounting for 2% of all cases, is the least common form. Type 4 (unclassified form) accounts for approximately 10% of cases. The organoaxial form (Type 1) is generally seen in middle-aged to elderly individuals; on the other hand the mesenteroaxial form (Type 2) is mostly encountered in childhood. Mesenteroaxcial form results in gastric ischemia more than organoaxial type volvulus 2,3.
Mesenteroaxial and the combined types are generally present with acute onset 2. Acute cases of gastric volvulus present with the Borchardt triad, that consists of epigastric pain, vomiting and the inability to install a nasogastric tube. Chronic cases mostly have an intermittent presentation of upper abdominal distension, gastro esophageal reflux or intermittent dysphagia. Symptoms on admission can change according to the patient?s age, disease progression rate, degree of rotation, and presence of obstruction?strangulation or perforation 3,6.
Idiopathic volvulus is less common (30%) and thought to be secondary to laxity of the perigastric (gastrohepatic, gastrosplenic, gastroduodenal or gastrophrenic) ligaments that allow the cardiac and pyloric ends to come closer especially when the stomach is full. And this new position is predisposing to volvulus. Secondary volvulus is more common (up to 86% of cases) , and is associated with para-oesophageal hiatus hernia, traumatic diaphragmatic hernia, diaphragmatic eventration, previous gastro-oesophageal surgery, including phrenic nerve palsy, and intrapleural adhesions 5.
The most challenging step in diagnosing acute gastric volvulus is the consideration of this diagnosis. Sometimes, hyperamylasemia and elevated serum alkaline phosphatase may be present. However, biochemical tests generally are not useful in diagnosis. The esophagus?stomach?duodenum passage images with barium contrast and CT scans are useful in the diagnosis. For prompt diagnosis, particularly in cases of acute onset, advanced clinical and radiologic experience is required 3,5.
Acute gastric volvulus presents as a retrocardiac air bubble or large air-fluid level in the chest on a chest X-ray. A barium contrast study showing obstruction of the stomach at the site of the volvulus can confirm the diagnosis. Since, acutely ill patients might not tolerate oral contrast and urgent diagnosis is important for surgical intervention; offering an immediate diagnosis with anatomical details CT scans become more important. There are reports in literature assert that CT should be the first choice of imaging as it avoids delay in diagnosis 2,6.
Gastric volvulus must be remembered, if an unusually high positioned stomach, an abnormal axis or an abnormal gastro esophageal junction-pylorus relationship is seen on CT images. Multiplanar reconstructed images ease displaying of torsion of the stomach, assisting in the confirmation of the diagnosis. Coronal images are the best to indicate close approximation of the gastro-oesophageal (GO) junction, and pyloric or abnormal antral folds that occur secondary to the volvulus 2.
CT scans might also be useful both in the detection of predisposing factors, like diaphragmatic defects, hernias, dense adhesions and other abnormalities associated with gastric volvulus, like wandering spleen, intrathoracic kidney, malrotation with asplenia. In addition CT has the ability to detect gastric pneumatosis and pneumoperitoneum which are suggestive of necrosis and perforation, to eliminate other extra-gastric or vascular causes of gastric ischemia and to detect other causes of abdominal pain if there is not a gastric volvulus present 2,5.
The treatment is surgery; laparotomy, de-rotation and internal fixation can all be performed. Gangrenous portions should be resected , if present. Recurrent volvulus can be prevented by anterior gastropexy where the greater curvature of the stomach is fixed to the anterior abdominal wall [5], and repair of the diaphragmatic defect is also important 6.
Conclusion
Acute gastric volvulus is an uncommon surgical emergency that should be kept in mind in patients who come to the emergency department with especially Borchardt symptoms. If gastric volvulus is one of the differential diagnoses, imaging studies become important. With its multiplanar demonstration of abnormal torsion, CT should be considered as first method of imaging for prompt diagnosis and surgical intervention. CT also provides valuable information about possible etiologies, and predisposing factors.
References
- Larssen K S, Stımec B, Takvam JA, Ignjatovıc D . Role of imaging in gastric volvulus: Stepwise approach in three cases. Turk J Gastroenterol. 2012; 23 (4): 390-3.
- Visser, Erasmus, Vawda & Partners, Port Elizabeth. Acute mesenteroaxial gastric volvulus on computed tomography : case report. S Afr J Rad. 2013; 17: 21-3.
- Altintoprak F, et al. A rare etiology of acute abdominal syndrome in adults: Gastricvolvulus ? Cases series. Int J Surg Case Reports. 2014; 5:731-4.
- Casella V, Avitabile G, Segreto S, Mainenti PP. CT findings in a mixed-type acute gastric volvulus. Emergency Radiol. 2011;18:483-6.
- Yi-Loong Woon C, Yaw-Fui Chung A, Albert Su-Chong Low A, Wai-Keong Wong. Delayed diagnosis of intermittent mesenteroaxial volvulus of the stomach by computed tomography: a case report. J Med Case Reports. 2008, 2:343.
- S Singham, B Sounness. Mesenteroaxial volvulus in an adult: time is of the essence in acute presentation: case report. Biomed Imaging Interv J. 2009; 5(3):e18.
|