Abstract
Duodenal lipomas are rare, benign tumors. When small in size, they are asymptomatic. When larger than 4 cm in particular they can cause symptoms such as pain or complications including intussusception and obstruction. Fluoroscopic imaging, endoscopic ultrasonography, computerized tomography and magnetic resonance imaging can be used in diagnosis.
Keywords :
Duodenal lipoma
, computerized tomography
, abdominal pain
Turkish Abstract
Duodenal lipomlar nadir, benign tümörlerdir ve küçük boyutlu olduklarında asemptomatiktirler. Özellikle dört cm den büyük olduklarında ağrı gibi semptomlara yada intusepsiyon, obstrüksiyon gibi komplikasyonlara neden olabilirler. Tanıda fluroskopik inceleme, endoskopik ultrasonografi, bilgisayarlı tomografi ve manyetik rezonans görüntüleme kullanılabilir.
Turkish Keywords :
, Duodenal lipom
, bilgisayarlı tomografi
, karın ağrısı
Introduction
Lipomas are slow-growing benign mesenchymal tumors that can derive from any location containing fat tissue. Corticosteroid use, obesity, diabetes, trauma and genetic factors have been implicated in the etiology1. Lipomas in the gastrointestinal tract are rare. They can be seen throughout the entire gastrointestinal tract, but are more common in the colon. Such patients are frequently asymptomatic and are identified incidentally during endoscopy, surgery or radiological imaging2. Computerized tomography (CT) and magnetic resonance imaging (MRI) are particularly important at differential diagnosis due to the characteristic density and signal characteristics of the fatty tissue3. Treatment can involve endoscopic techniques or open surgery2. We describe a duodenal lipoma identified in a patient presenting to the emergency department with pain in the upper right quadrant, together with imaging findings.
Case Report
A 47-year-old man presented to our hospital emergency department with pain in the upper right quadrant. His medical history was unremarkable except for inguinal surgery three years previously. He reported symptoms of dyspepsia for the previous approximately one year. He stated that these had worsened in the last two days and described severe pain in the upper right quadrant.
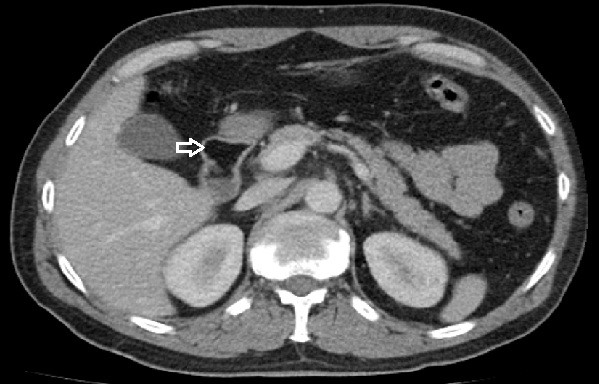
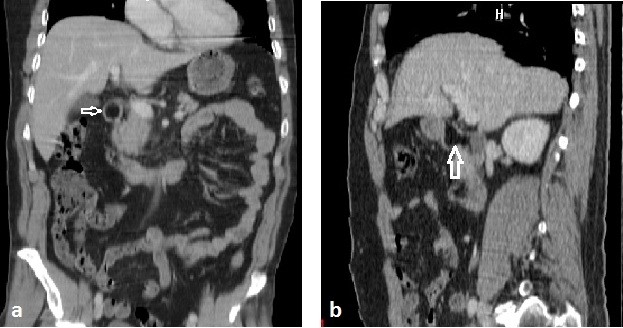
Routine blood count and biochemistry tests were normal. No pathology was determined at direct abdominal x-ray. Abdominal CT was performed with preliminary diagnoses of pancreatitis and gastrointestinal perforation. Lesion compatible with fat tissue with a density of -96 HU was determined inside the duodenal lumen (Figure1 and 2).
Lipoma was diagnosed based on radiological imaging. Elective surgery was recommended after medical treatment, and the patient was discharged.
Discussion
Gastrointestinal tract lipomas are rare. The prevalence is listed as 64% in the colon, 26% in the small intestine, 4% in the duodenum, 3% in the stomach and 2% in the esophagus4. Good CA. reported duodenal lipoma in 17 cases in a study of 659 patients with small bowel tumor5. A relation has been reported between symptom development and size of tumor in previous cases in the literature. Small lipomas are generally asymptomatic and are frequently diagnosed incidentally during radiological imaging or endoscopy. Symptomatic cases are generally larger than 4 cm4,6. The most common symptoms are abdominal pain, nausea and vomiting.
Complications such as obstruction, intussusception and bleeding have been reported in some cases. No complication was determined with imaging findings in our patient with pain in the upper right quadrant. Duodenal lipomas are benign in character, and no malignant transformation has been reported6. Ovoid/polypoid lesions are covered by normal mucosa at endoscopic examination. Since 90% of cases are submucosal in location, normal mucosa findings are observed in endoscopic biopsies7. The pillow sign observed during endoscopy is an indirect finding for lipoma8.
Although used more rarely today, upper gastrointestinal tract fluoroscopy can assist with diagnosis. Findings appear as well-marginated, non-ulcerated filling defects. These findings are suggestive of a benign lesion, but are not specific for lipoma9. Endoscopic ultrasonography findings are homogeneous, hyperechoic lesions of submucosal origin8.
Lipomas appear as homogeneous, well-marginated and capsuled lesions with regular borders at CT and MRI. Thin, fibrous septae may rarely be observed. Density values for fat tissue between -50 and -150 HU at CT or a hyperintense signal character on T1 and T2 weighted images at MRI are suggestive of lipoma3,10. A hypointense signal at MRI or on fat-suppressed sequences is important in diagnosis. Liposarcoma must be considered in the presence of thick septa, non-fat structures, heterogeneity or contrast involvement10.
Small, asymptomatic lesions should be monitored. Endoscopic procedures are generally preferred today in symptomatic cases. Snare, endoloop, unroofing, subtotal resection or submucosal dissection techniques can be used at endoscopy11. The localion and size of the lesion influence the decision regarding which technique should be used. Endoscopic treatment may be difficult in lesions located in the second segment of the duodenum or more distally, or in large lesions11.
In conclusion, duodenal lipomas are rare, frequently asymptomatic and benign tumors. Diagnosis is often made using sectional imaging techniques such as CT and MRI.
References
- Mesolella M et al. Parotid Lipoma: A Case Report. Case Reports in Clinical Medicine 2014; 3: 437-42.
- Aydin HN, et al. Safe techniques for endoscopic resection of gastrointestinal lipomas. Surg Laparosc Endosc Percutan Tech 2011; 21: 218-222.
- Öztürk E, et al. Duodenal Lipom: Bilgisayarlı Tomografi Bulguları. Anatol J Clin Investig 2009:3(1):50-51
- Parmar AK, et al. Laparoscopic management of a large duodenal lipoma presented as gastric outlet obstruction. JSLS. 2013 Jul-Sep;17(3):459-62
- Good CA. Tumors of the small intestine. Am J Roentgenol Radium Ther Nucl Med 1963;89:685?7
- Vinces FY, et al. Gastroduodenal intussusception secondary to a gastric lipoma. Can J Gastroenterol 2005;19:107-8.
- Huang WH, et al. Endoloop-assisted unroofing for the treatment of symptomatic duodenal lipomas. Gastrointest Endosc 2008; 68: 1234-1236.
- Aydın A, et al. Üst gastrointestinal sistem lipomları: 33 Olgunun irdelenmesi. Endoskopi dergisi 2009; 17(1):12-3
- Abu Daff SN, Abu Daff NS. Laparoscopic enucleation of a duodenal lipoma, with review of the literature. Saudi Med J 2008;29:455?7.
- Tüzün M, Hekimoğlu B. Lipomların nadir lokalizasyonları: BT ve MR görünümleri. Türk Radyoloji Derg 2016; 35: 77-80.
- Yaman İ, Derici H, Paksoy S. Endoskopik snare polipektomi uygulanan semptomatik duodenal lipom olgusu. Ulusal Cer Derg 2014; 30: 103-5.
|