Abstract
A 66-year old man presented to emergency department with a complaint of cough and chest discomfort after smoke inhalation. He was diagnosed as acute myocardial infarction and showed high carbon monoxide (CO) levels. Angiography confirmed diagnosis. CO intoxication must be considered in patients with acute coronary syndromes and supplemental oxygen therapy with non-rebreathing mask is essential for these patients.
Keywords :
Carbon monoxide
, Myocardial infarction
, Oxygen
Turkish Abstract
Altmış altı yaşındaki erkek hasta acil servise duman inhalasyonu sonrasında öksürük ve göğüs ağrısı yakınması ile başvurmuştur. Hasta, akut miyokard infarktüsü tanısı almış ve yapılan tetkikte yüksek karbonmonoksit seviyeleri ölçülmüştür. Koroner anjiyografi ile tanı doğrulanmıştır. Karbonmonoksit zehirlenmeleri, akut koroner sendromlu hastalarda değerlendirilmelidir ve bu hastalar için oksijen destek tedavisi temel basamaktır.
Turkish Keywords :
, Karbon monoksit
, Miyokard infarktüsü
, Oksijen
Introduction
Acute coronary syndromes are the most frequent mortality causes in both male and female adults. Intoxications are important triggers of acute myocardial infarction (AMI) and cardiac arrest. We reported an AMI case triggered by carbon monoxide (CO) intoxication.
Case Report
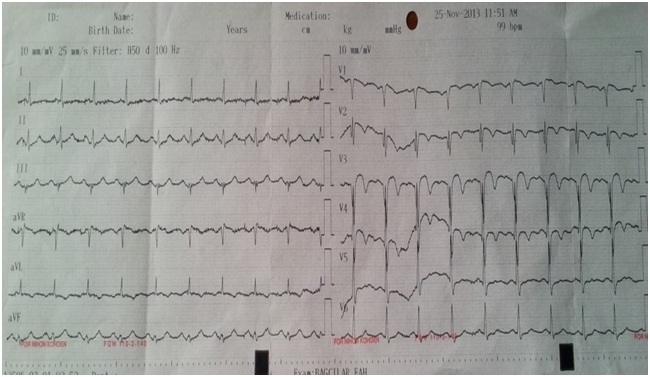
A 66-year-old male was admitted to the emergency department (ED) with complaints of cough, dyspnoea, head ache, and chest discomfort. His complaints were started after exposure of stove smoke two hours before admission. The patient was awake (GCS: 15), and denied any chronic disease such as cardiovascular disease. He also denied cigarette and alcohol consumption. Family history was negative. His vital signs were BP: 110/70 mmHg, pulse rate: 102 bpm (regular), temperature: 37.2 °C and SaO2: 89 %. Heart and lung auscultation and systemic examination did not show any abnormality. Initial ECG showed ST elevation and biphasic T waves in leads V2-4 and T wave inversion in lead aVL (Figure 1).
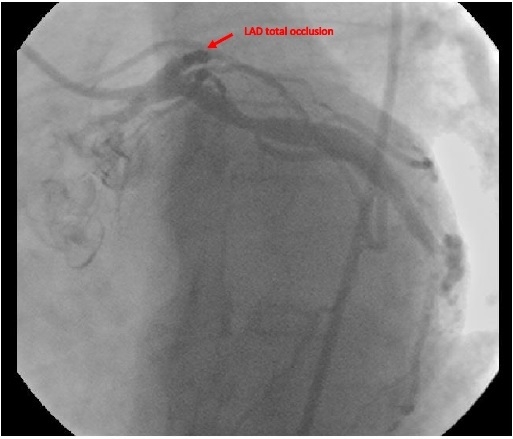
Aspirin (300 mg, per oral, non-enteric coated) was administered, heparin infusion was initialised, and supplemental oxygen started via nasal cannula. Laboratory values revealed a haemoglobin value of 15.2 (ref: 13.3-17.2) mg/dl; WBC: 15.9 x10³ /mm³ with 85.7 % (ref: 40-74) neutrophils. The platelet count was 245x10³ /mm³ (ref: 130-400) and troponin I was 7.49 ng/ml (ref: 0.001-006). Arterial blood gas values, with room air, showed a pH of 7.34; PCO? of 44.2 mm Hg (ref: 35-46); PO? of 56.8 mm Hg (ref: 80-100), and COHb: 9.5% (ref.: 0.5-2.5). Supplemental oxygen therapy continued with non-rebreather oxygen mask because of high CO level. The patient has undergone emergent coronary angiography and a total occlusion of proximal left anterior descending artery (LAD) was confirmed. There was no lesion in the left main coronary artery (LMCA), there were non-obstructive plaque formations in the circumflex artery (CX) and right coronary artery (RCA), blood flow appeared normal in these both arteries (Figure 2).
We tried to apply balloon angioplasty but failed to maintain coronary blood flow. The patient refused coronary artery by-pass graft surgery (CABG). He was admitted to the intensive care unit, medical therapy was planned, troponin levels regressed, and discharged without any complication. The patient could not be reached for follow-up.
Discussion
Carbon dioxide intoxication is a mortal clinical situation and it is one of the most frequent intoxications all over the world. Syncope, headache, changes in level of consciousness, nausea, vomiting are frequent complaints but different clinical conditions even death can occur. The basic pathophysiology of CO intoxication is the higher affinity of CO to hemoglobin (Hb) than oxygen, constitution of carboxyhemoglobin (COHb) after binding to Hb, low oxygen carry capacity of COHb, and impaired tissue oxygen delivery to the tissues 1. Tissues with high oxygen demand such as brain and heart are tend to be affected more than other tissues 1.
Cardiac involvement can result in cardiomyopathy, myocardial infarction (MI), arrhythmias, cardiogenic shock and sudden death. There are several MI cases due to CO intoxication in the literature 1-8. However, most of them showed ST-elevation myocardial infarction (STEMI), CO levels and ECG changes has not been associated 9. In our case total occlusion of LAD was detected but recanalization attempts failed and CABG was not applied. These suggest that CO intoxication could cause an imbalance between myocardial oxygen supply and/or demand that results in myocardial injury in patients with pre-existing coronary artery disease.
Possible harmful effects of supplemental oxygen therapy in acute coronary syndromes have been considered 10. However, treatment of COHb is 100% oxygen therapy until the symptoms resolve, and COHb levels decrease below 5-10%1 . In acute coronary syndrome patients with CO intoxication, oxygen therapy is essential and must be initialised as soon as possible.
Carbon dioxide intoxication is a mortal condition that can mimic a wide range of clinical conditions. Diagnosis is usually based on clinical suspicion and detection of COHb levels in blood gas analyses. STEMI due to CO intoxication does not differ in treatment but 100% oxygen therapy must be initialised as soon as possible independently from oxygen saturation levels.
References
- Lippi G, et al. Pathophysiology, clinics, diagnosis and treatment of heart involvement in carbon monoxide poisoning. Clin Biochem. 2012;45(16-17):1278-85.
- Dziewierz A, et al. Primary angioplasty in patient with ST-segment elevation myocardial infarction in the setting of intentional carbon monoxide poisoning. J Emerg Med. 2013;45(6):831-4.
- Isik T, et al. ST-elevation myocardial infarction after acute carbon monoxide poisoning. Anadolu Kardiyol Derg. 2012;12(3):278-9; author reply 9.
- Kim S, et al. A case of acute carbon monoxide poisoning resulting in an ST elevation myocardial ınfarction. Korean Circ J. 2012;42(2):133-5.
- Szponar J, et al. [Myocardial infarction secondary to carbon monoxide poisoning--a study of two cases]. Przegl Lek. 2011;68(8):527-9.
- Gonullu H, et al. ST elevation myocardial ınfarction due to carbon monoxide poisoning. Eurasian J Med. 2011;43(2):125-8.
- Hsu PC, et al. Acute carbon monoxide poisoning resulting in ST elevation myocardial infarction: a rare case report. Kaohsiung J Med Sci. 2010;26(5):271-5.
- Tucciarone M, et al. Myocardial infarction secondary to carbon monoxide poisoning: an uncommon presentation of a common condition. Case report and review of the literature. Am J Ther. 2009;16(5):462-5.
- Hajsadeghi S, et al. Electrocardiographic findings and serum troponin I in carbon monoxide poisoned patients. Acta Med Iran. 2012;50(3):185-91.
- Shuvy M, et al. Oxygen therapy in acute coronary syndrome: are the benefits worth the risk? Eur Heart J. 2013;34(22):1630-5.
|