Abstract
Psoas abscess (PA) is a rare clinical presentation, often with nonspecific clinical symptoms and signs. Emergency physicians should consider psoas abscess in patients presenting with fever of unknown origin, low back pain, and/or lower extremity pain. The diagnosis depends on an accurate history and comprehensive physical examination with the raised suspicion of psoas abscess. Percutaneous or open surgical drainage and antibiotic therapy remain the major treatment modalities. Here, we report a case of 89-year-old male who was admitted with bilateral lower extremity and low back pain. The psoas abscess was detected on his magnetic resonance imaging (MRI) and the patient was treated with antibiotic therapy plus percutaneous drainage with the insertion of an ultrasound-guided pigtail catheter. Escherichia coli was isolated from the pus culture. The urinary tract infection was considered to be the possible origin of the psoas abscess in the patient.
Keywords :
Escherichia coli
, Low back pain
, Percutaneous drainage
, Psoas abscess
Turkish Abstract
Psoas absesi, spesifik olmayan klinik semptom ve bulgularla kendini gösteren nadir klinik bir durumdur. Acil tıp hekimi, bilinmeyen orijinli ateş, bel ağrısı ve/veya bacak ağrısı ile başvuran hastalarda psoas absesini akla getirmelidir. Tanı, uygun bir anamnez ve kapsamlı fizik muayene ile artmış psoas absesi şüphesi varlığına bağlıdır. Esas tedavi yöntemleri, antibiyotik terapi ve perkutan veya açık cerrahi drenajdır. Biz, bel ve bacak ağrısı ile kabul edilen 89 yaşında erkek olguyu sunduk. Magnetik rezonans görüntüleme ile hastanın psoas absesi saptandı. Hasta antibiyotik terapi ve ultrason klavuzluğunda pigtail kateter yerleştirilerek perkutan drenaj ile tedavi edildi. Cerahat kültüründen Escherichia coli izole edildi. Hastada, psoas absenin muhtemel orijini üriner yol enfeksiyonu olarak düşünüldü.
Turkish Keywords :
, Escherichia coli
, Bel ağrısı
, Perkütan drenaj
, Psoas abse
Introduction
Psoas muscle abscess is a pyogenic inflammation of iliopsoas muscle. It may be secondary to septicemia or another disease process around the iliopsoas muscle 1. It is a rare clinical condition with high mortality and morbidity. Although it has nonspecific clinical symptoms and signs, increased use of abdominal computerized tomography (CT) or magnetic resonance imaging (MRI) to evaluate septic patients with unknown foci makes the diagnosis easier.
Psoas abscess (PA) may be classified as primary or secondary depending on the etiology of infection 2. Primary PA occurs as a result of haematogenous spread of an infection from an occult source especially in young adults. It may be presented in patients with diabetes mellitus, intravenous drug abuse, AIDS, renal failure and immunosuppresion 2. The classical clinical triad is fever, back pain and limp pain, seen in only 30% of the patients. Abdominal pain, malaise, nausea, and weight loss are the other symptoms 3. Secondary causes are direct spread of the infection from adjacent structures, most commonly seen in Crohn?s disease or any surgical or instrumentation of adjacent anatomical structures, seen in elderly patients 4.
Treatment of PA with antibiotherapy alone is not commonly reported in the literature. Open or percutaneous drainage plus antibiotheraphy are the most effective treatment method for PA 4-6. As open drainage method may be associated with significant morbidity in the septic patients, the less invasive drainage methods such as percutaneous catheter drainage under radiological guidance has become the preferred treatment method.
We report a 89-year-old male who was admitted with limp and back pain. Psoas abscess was detected on MRI, and treated with antibiotherapy plus percutaneous drainage with the insertion of an ultrasound-guided pigtail catheter.
Case Report
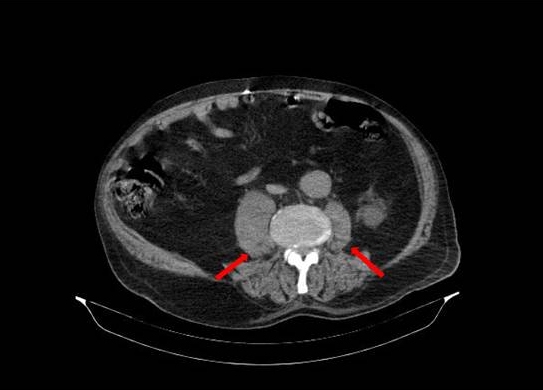
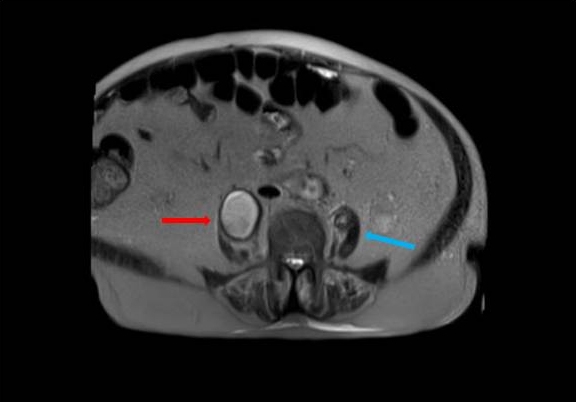
A 89-year-old male patient was presented to the Emergency Department (ED) with limp and back pain. He was admitted to hospital three weeks ago because of urinary tract infection. The patient had a history of type II diabetes, Alzheimer?s disease, hypertension, congestive heart failure and benign prostatic hyperplasia. He had no history of tuberculosis. His vital signs were stable. Physical examination was within normal limits. Laboratory studies demonstrated no abnormal values except mildly elevated creatinine level as 1.3 mg/dL. WBC count was 7.900 K/uL. Non-contrast enhanced CT scan of the lumbar spine was obtained and revealed normal spinal cord and vertebral column. Patient?s symptoms improved and he was discharged from ED. The following day, he presented to ED again with the same complaints. He was referred to orthopedic surgery because of ongoing pain and an urgent lumbar spine MRI scan was performed. MRI scan demonstrated multiple psoas abscesses - the biggest was 4.5x7.7 cms- on both sides and left sided iliopsoas bursitis (Figure1 and Figure2).
Percutaneous drainage was performed with the insertion of an ultrasound-guided pigtail catheter and patient was admitted to infectious disease ward. The patient was treated with intravenous antibiotics. A pus culture showed a mono-organism -Escherichia coli (E. coli) and Enterococcus was isolated from blood culture in the patient. Blood, urine and pus cultures were negative for ARB. He was discharged after 51 days without any complications.
Discussion
Pyogenic PA may be divided into two groups according to its etiology. Primary PA occurs due to hematogenous or lymphatic spread of etiologic agent from a distant site, and secondary PA occurs from an adjacent infectious or inflammatory process by direct expansion 4. The leading infectious agents in patients with PA are methicillin-susceptible Staphylococcus aureus (27%), and Escherichia coli (18%) 7. Primary PA is most probably secondary to an unrecognized staphylococcic infection, 8 however, secondary PA is generally caused by enteric pathogens that arise from intraabdominal region, particularly intestinal origin 2,4,9,10. Urinary tract infection and instrumentation of the renal region may be an origin for secondary PA 4,7,11,12. As the etiologic agents in our patient were Escherichia coli and Enterococcus, and the history of urinary tract infection was positive three weeks ago, he was evaluated as secondary PA. Other causes of secondary PA such as Crohn?s disease, appendicitis, ulcerative colitis, diverticulitis, colorectal carcinoma, hepatocellular carcinoma, spinal tuberculosis, infectious sacroiliitis, endocarditis, instrumentation or catheterization of renal tract and/or femoral artery were not present in our patient.
The initial diagnosis of PA, based on an accurate history and comprehensive physical examination, must be made with the raised suspicion of PA. History should include the progression of symptoms as well as contributing factors such as gastrointestinal, urogenital, and musculoskeletal disorders 4. The classic triad of PA may only be present in 1/3 of cases 3. Nonspecific symptoms such as low-grade fever and malaise may progress into more specific symptoms like abdominal/flank discomfort, pain on movement of the hip secondary to irritation of the muscle belly, externally rotated and flexed hip, referred pain from the nerve roots L2-L4, which supply the psoas muscle 13,14. Appropriate diagnostic modalities for PA include laboratory (i.e. full blood count, C-reactive protein, erythrocyte sedimentation rate, blood cultures) and radiologic investigations (i.e. ultrasound, CT scan, MRI). Laboratory studies of pus and blood cultures were diagnostic in our patient. One of the common causes of PA in developing countries is spinal tuberculosis-Pott?s disease, which should be ruled out in all patients. Our patient showed negative culture results of ARB.
MRI has many advantages than CT because of better discrimination of soft tissues and ability to visualize the abscess wall and the surrounding structures 15,16. The PA in our patient was detected on MRI. Abscesses with low attenuation and no air-fluid presentation cannot be determinated by CT scan and also non-contrast enhanced CT scan modalities are inappropriate for detecting abcesses as seen in our patient. Zissin et al. reported that even though non-classical presentations were present, the CT scan was an effective imaging modality for diagnosing PA. The present series proves the importance of the diagnostic and therapeutic role of CT scans 17.
An ultrasound-guided percutaneous drainage by pigtail catheter is possible for diagnosis and treatment as performed in our patient. The major limitation of ultrasound-guided percutaneous drainage is its technical difficulties to drain abscesses with multiple separations, small abscesses, and abscesses located in unreachable sites 6,18,19. Many small abscesses may be treated with antibiotics alone 20. The possible therapeutic approach of abscesses which do require drainage may be aspiration via CT guidance and antibiotic therapy 4,5.
In secondary PA, it is wise to start broad spectrum antibiotic treatment that covers S.aureus and also gram negative and anaerobic bacteria 2,4,5,14,18-20. Some authors believe that targeted antibiotherapy alone will sufficiently treat abscesses up to 6 cm diameter 20. Although, the majority of PA may be aspirated effectively by CT guided percutaneous drainage, 5surgical drainage may be preferred in some conditions 4. In patients with intra-abdominal pathology such as complex Crohn?s disease or diverticulitis and also failure of the CT guided percutaneous drainage, surgery is indicated 14,19-21.
Psoas abscess is a rare disease. The clinical presentation of psoas abscess is often variable and non-specific. Emergency physicians should always be alert about the situations such as prolonged fever of unknown origin, back pain, and/or limp pain. Percutaneous drainage remains the primary initial treatment modality for psoas abscess. Surgical drainage may be preferred, if necessary. Early management and drainage of the abscess reduce the morbidity and mortality.
References
- Huang JJ, et al. Acute pyogenic iliopsoas abscess in Taiwan: clinical features, diagnosis, treatment and outcome. J Infect. 2000;40:248?55.
- Ricci MA, Rose FB, Meyer KK. Pyogenic psoas abscess: worldwide variations in etiology. World J Surg. 1986;10: 834?43.
- Chern CH, et al. Psoas abscess: making an early diagnosis in the ED. Am J Emerg Med. 1997;15:83-8.
- Shields D, Robinson P, Crowley TP. "Iliopsoas abscess?A review and update on the literature." Int J Surg. 2012; 9:466-69.
- Navarro Lopez V,et al. GTI-SEMI Group. Microbiology and outcome of iliopsoas abscess in 124 patients. Medicine 2009;88:120-30.
- Dinc H,et al. Image guided percutaneous of tuberculous iliopsoas and spondylodiskitic abscesses: midterm results. Radiology. 2002;225:353-8.
- Lai YC, et al. An update on psoas muscle abscess: An 8-year experience and review of literature. Inter J Gerontol. 2011;5:75-79.
- Bresee JS, Eowards MS. Psoas abscess in children. Pediatr Infect Dis J. 1990;9:201?6.
- Leu SY, et al. Psoas abscess: changing patterns of diagnosis and etiology. Dis Col Rectum. 1986; 29:694?8.
- Santaella RO, Fishman EK, Lipsett PA. Primary vs secondary iliopsoas abscess: presentation, microbiology, and treatment. Arch Surg. 1995;130:1309?13.
- Taiwo B. Psoas abscesses: a primer for the internist: case report. South Med J. 2001;94:78-80.
- Van Dongen LM, Lubbers EJC. Psoas abscess in Crohn?s disease. BJS. 2005:589-90.
- Wong JG. The psoas signs. Well-described but often forgotten physical examination findings of iliopsoas inflammation. N C Med J. 1993;54:598-600.
- Ricci MA, Meyer KK. Psoas abscess complicating Crohn?s disease. Am J Gastroenterol. 1985;80:970-7.
- 15. Wall SD,et al. Magnetic resonance imaging in the evaluation of abscesses. AJR. 1985;144:217-22.
- Rieber A,et al. Diagnostic imaging in Crohn?s disease: comparison of magnetic resonance imaging and conventional imaging methods. Int J Colorectal Dis. 2000;15:176-81.
- Alvi A R, Rehman ZU, Nabi ZUGR. Pyogenic psoas abscess: case series and literature review. Tropical Doctor. 2010; 40:56-58.
- Lee YT, et al. Psoas abscess: a 10 year review. J Microbiol Immunol Infect 1999;32:40-6.
- Gupta S,et al. Iliopsoas abscesses: percutaneous drainage under image guidance. Clin Radiol. 1997;52:704-7.
- Yacoub W, et al. Psoas abscess rarely requires surgical intervention. Am J Surg. 2008;196: 223-7.
- Lobo DN, et al. Psoas abscess complicating colonic disease: imaging and therapy. Ann R Coll Surg Engl . 1998;80:405-9.
|