Abstract
Paediatric trigger finger is a rare condition, being ten times less common then paediatric trigger thumb. Trigger digit in children are predominantly present with flexion deformity and a nodule in metacarpophalangeal joint. This rare condition in children, trigger finger, was occasionally reported to be bilaterally or to be equally in male and female patients. Although described as congenital, some authors did not agree with and they did not found any trigger fingers in their study populations of newborn children. Treatment can be either conservative or surgical. Here we reported two cases of patients with trigger fingers, one of them treated by conservative methods, and the other treated surgically.
Keywords :
Trigger finger
, A1pulley
, Flexion deformity
Turkish Abstract
Pediatrik tetik parmak, nadir bir durumdur ve pediatrik tetik baş parmaktan 10 kez daha az görülmektedir. Çocuklardaki tetik parmak, sıklıkla fleksiyon deformitesi ve metakarpofalangeal eklemde bir nodul ile ortaya çıkar. Çocuklardaki bu az rastlanan durum, tetik parmak, nadiren bilateral olmaktadır ve erkek ve kadınlarda eşit oranda ortaya çıkmaktadır. Konjenital olarak tanımlanmasına rağmen, bazı otörler buna katılmamaktadırlar ve yenidoğanlardan oluşan kendi çalışma gruplarında tetik parmağa rastlamamışlardır. Tedavi, konservatif veya cerrahi olabilir. Burada, bir tanesi cerrahi olarak, diğeri konservatif yollarla tedavi edilen iki tetik parmak vakası bildirdik.
Turkish Keywords :
, Tetik parmak
, A1 yastıkçık
, Fleksiyon deformitesi
Introduction
Trigger finger is one of the most common hand diseases seen in female patients at the ages of 50-60 1-2. However, this is a rare condition in pediatric population. Although described as congenital, some authors did not agree with and also they did not find any trigger fingers in their study population of newborn children 3-5. The prevalence among all children was 1/20004. The pathology of disease is generally the locking of flexor tendon over A1 pulley due to narrowing of the canal or bulging of tendon. Etiology is not clear and sometimes it is associated with other congenital anomalies 6. Treatment can be either conservative or surgical. The most common conservative treatments performed are passive flexion-extension stretching of the fingers and splint therapy 7.
In this study, we reported two cases of patients with trigger fingers, one of them was treated by conservative methods, and the other was treated surgically.
Case Report
Case 1:
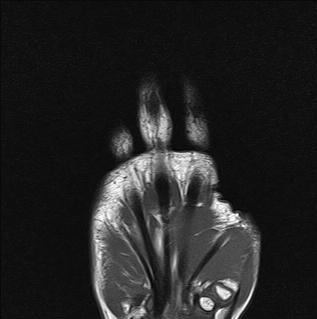
A 9-year-old boy was seen with a complaint of difficulty in extending the first and second fingers of right hand and grasping the objects. His mother stated that restriction of motion had been noticed at two months after birth and grasping difficulty had worsened over the last 6 months. The physical examination showed triggering in second finger and minimally restricted finger extension of both two fingers. The thumb flexion and abduction strength was 4/5. All other joint examination and systemic examination was in normal ranges. Laboratory tests including complete blood cell count, erythrocyte sedimentation rate, C - reactive protein and total biochemistry analysis were in normal ranges. Mild increase in echogenicity of flexor tendons was observed on superficial tissue ultrasound. No significant pathology was detected by magnetic resonance imaging (MRI) (Figure1).
The patient was diagnosed clinically as having trigger finger and was recommended to do passive and active range of motion (ROM), stretching and strengthening exercises. At the third month visit, the patient was able to flex and extend his finger through normal ranges of motion and without triggering.
Case 2:
A 4-year-old boy was seen with a complaint of triggering in the fourth fingers of both hands and difficulty in opening and closing the hands. His parents stated that triggering had been noticed at seven months after birth, and despite physical therapy, his complaints persisted. All systemic examination was normal except triggering in both fourth fingers and bilateral palmar nodules. Laboratory tests consisting of complete blood cell count, erythrocyte sedimentation rate, C - reactive protein and total biochemistry analysis were in normal ranges. No significant pathology was observed on ultrasound and MRI of both hands (Figure 2).
The patient was diagnosed as having trigger finger clinically and was recommended to do passive and active ROM, stretching and strengthening exercises. At the six month visit the complaints were resisting. Therefore, the patient was evaluated by plastic and reconstructive surgery department and treated surgically. For both fourth fingers A1 pulleys were released. After the operation, his complaint of triggering disappeared.
Discussion
Paediatric trigger finger is a rare condition, being ten times less common then paediatric trigger thumb. Trigger digit in children are predominantly present with flexion deformity and a nodule in metacarpophalangeal joint. This rare condition in children, trigger finger, was occasionally reported to be bilaterally or to be equally in male and female patients. Previously, in a study, a slight female predominance and 16% bilateral involvement were reported 4. In these two cases, the patients were both male and while one of them had bilaterally trigger fingers, the thumb and second digit of the other patient were triggering.
The fact, how to treat these children, is controversial. While many authors suggest surgical treatment 4,7,8, the others recommend physiotherapy in the treatment of trigger fingers in children 9. In addition, spontaneous resolution of trigger thumbs was also reported in about 30% of the patients 10. While one of these two cases improved spontaneously, the other was treated surgically.
The underlying mechanisms and how to treat trigger finger in children are controversial. Further studies with great patient population with long follow-up periods are warranted to answer these questions.
References
- Yang TH, et al. Clinical and pathological correlates of severity classifications in trigger fingers based on computer-aided image analysis. Biomed Eng Online. 2014;13:100.
- Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am. 2006;31:135-46.
- Slakey JB, Hennrikus WL. Acquired thumb flexion contracture in children: congenital trigger thumb. J Bone Joint Surg Br. 1996;78:481-3.
- Leung OY, et al. Trigger thumbs in children: results of surgical release. Hong Kong Med J. 2011;17:372-5.
- Moon WN, Suh SW, Kim IC. Trigger digits in children. J Hand Surg Br. 2001;26:11-2.
- Herdem M, et al. Clinical analysis of the trigger thumb of childhood. Turk J Pediatr. 2003;45:237-9.
- De Luna V, et al. Multiple congenital bilateral trigger digits in a 2-year-old child: case report. Open Orthop J. 2013;7:75-7.
- Cardon LJ, Ezaki M, Carter PR. Trigger finger in children. J Hand Surg Am. 1999;24:1156-61.
- Kelle B. Trigger finger in childhood: A case report. J PMR Sci. 2012;15:61-3.
- Dinham JM, Meggitt BF. Trigger thumbs in children. A review of the natural history and indications for treatment in 105 patients. J Bone Joint Surg Br. 1974;56:153-5.
|