Abstract
Plasmacytomas are rare tumors constituting 1% of all head and neck (HN) neoplasms. Most of HN plasmacytomas in the literature were presented as single case report and according to best of our knowledge, such a high number of plasmacytomas in the HN region with their Positron emission tomography/Computed tomography (PET/CT) findings have never been published before. In our four cases, we aim to underline the efficiency of PET/CT in diagnosis of HN plasmacytomas and also demonstrate the superiority of PET/CT in evaluation of radiotherapy response.
Keywords :
Computed tomography
, Head and neck
, Plasmacytoma
, Positron emission tomography
Turkish Abstract
Baş ve boyun (BB) plazmositomları nadir görülen tümörler olup, tüm BB neoplazilerinin %1?ini oluşturur. Literatürdeki birçok BB plazmositomu tek olgu sunumu şeklinde sunulmuş olup bildiğimiz kadarıyla pozitron emisyon tomografisi/bilgisayarlı tomografi (PET/CT) bulgularıyla sunulan bu kadar çok sayıda BB plazmositomu daha önce yayınlanmamıştır. Bu dört olgudaki amacımız PET/ CT?nin BB plazmositom tanısındaki etkinliği vurgulamak ve radyoterapiye olan cevabı değerlendirmedeki üstünlüğünü göstermektir.
Turkish Keywords :
, Bilgisayarlı tomografi
, Baş ve boyun
, Plazmositom
, Pozitron emisyon tomografisi
Introduction
Plasmacytoma is characterized by proliferation of neoplastic plasma cells in non-osseous tissues and it may occur as a primary extramedullary plasmacytoma (PEM), or in the process of multipl myeloma (MM), primary amyloidosis and monoclonal gammopathy of undetermined significance. PEM is a rare tumor, constituting 4% of all plasma cell tumors. PEM is differantiated from MM by the absence of renal failure, anemia, elevated serum calcium levels, bone marrow plasmocytosis and positive bone surveillance in X-ray 1, 2.
Either in primary form or in the subgroup of secondary form, the most common presentation of head and neck (HN) plasmacytoma is a submucosal mass in the upper airways. Nasal cavity, nasopharynx, oropharynx, larynx and paranasal sinuses are the common regions, which are often involved in this disease and this rare tumor constitutes only 1% of all HN tumors 3, 4.
Skeletal survey that covers axial, appendicular skeleton and head bones is the first preferred imaging modality, since it is advantageous over the other imaging modalities in demonstration of lytic bone lesions of MM . On the other hand X-ray has a limited value in evaluation of the diagnosis and treatment response, because at least 40-60% mineral loss is required for the bone lesions to be apparent in X-ray and direct radiography seldomly reflects the healing of the lytic bone lesions after treatment 5. Magnetic resonance imaging (MRI) is successful in assessment of bone marrow, soft tissue and in demonstration of potential complications such as spinal cord compression. With the relatively new MRI sequences such as dynamic post-contrast MRI and diffusion MRI, tumor burden can be effectively calculated 6. Positron emission tomography-Computed tomography (PET/CT) is superior over conventional imaging modalities, since it can detect early bone marrow invasion and it is highly effective for revealing extramedullary lesions and also for assessment of treatment response (e.g. chemotherapy, radiotherapy) 7, 8.
In the literature, HN plasmacytomas were mostly presented as single case report. According to best of our knowledge, PET/CT findings of HN plasmacytomas with such high number of cases have not been published before. The aim of this study is to present PET/CT findings (before and after radiotherapy) of four cases, who were pathologically confirmed to have HN plasmacytomas.
Case Report
Patients
Four cases, referred to the ear, nose and throat (ENT) clinic between February 2010 and February 2013 with several complaints were undergone biopsy after physical and radiological examination. Following the histopathological diagnosis of plasmacytoma, all patients underwent PET/CT examination in order to stage the disease before radiotherapy. Six months after radiotherapy, a control PET/CT was performed. The demographic features of the patients, the origins of the plasmacytomas, the measurements of the three dimensional tumor lengths (craniocaudal x transverse x anteroposterior) and maximum standardized uptake value (SUVmax) of each lesions before and after radiotherapy were recorded. The patients or their attendants were informed and the informed consents were obtained before PET/CT examination. The characteristics of the patients before and after radiotherapy, the three dimensional tumor lengths (in centimeter) of each plasmacytomas and the SUVmax values ??were summarized in Table 1.
Case 1
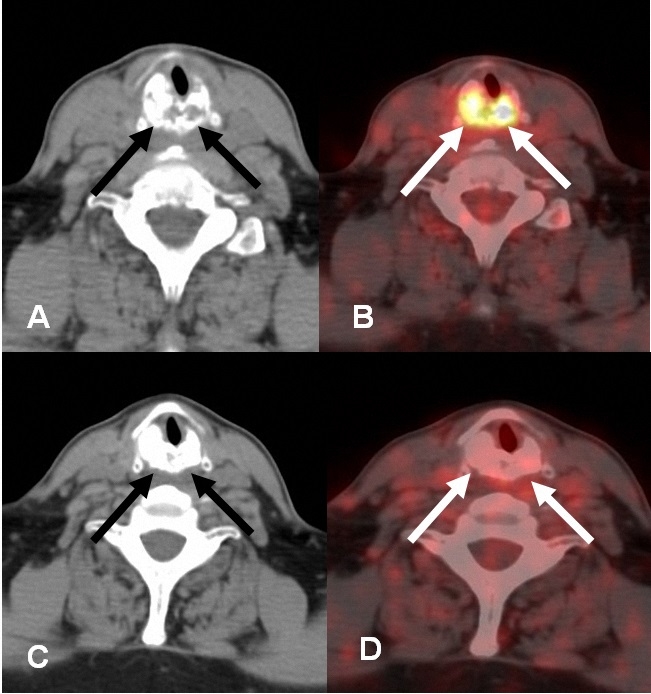
A 65-year-old male was admitted to the ENT clinic because of progressive hoarseness and shortness of breath, started 3 months before. No palpable mass was detected in the neck during physical examination. Laryngoscopic examination revealed a mass that narrowed air column in the infraglottic space from right posterolateral direction. However, there was no ulceration, inflammation or polypoid lesion on the mucosal surface. A biopsy was performed in the same session. The histopathological diagnosis was consistent with plasmacytoma and following the diagnosis, he underwent PET/CT for staging. On the initial PET/CT, an expansile mass involving arytenoid cartilages with both lytic and sclerotic changes was detected (Figure 1. a, b). Six months after radiotherapy, the SUVmax of the plasmacytoma in the arytenoid cartilage decreased from 11 to 1.7 (Figure 1. c, d). However, the lengths of the laryngeal plasmacytoma did not change dramatically (Table 1).
Case 2
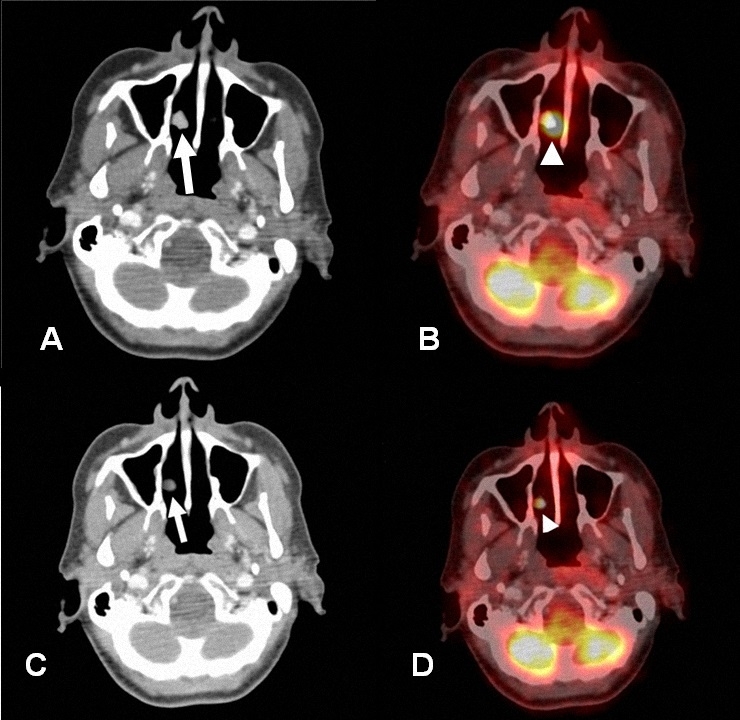
A 63-year-old female patient was admitted to the ENT clinic with long-standing complaints of nasal obstruction. She described nasal discharge, but there was no history of epistaxis. No palpable mass was detected in the neck during physical examination. She underwent endoscopic evaluation to investigate the reason of nasal obstruction. The examination showed a polypoid mass in the right nasal cavity. Following the detection of the solid mass, a biopsy was performed. The diagnosis of a nasal cavity plasmacytoma was made. First PET/CT examination revealed a solid mass originating from right posterior aspect of nasal septum with a SUVmax of 20.4 (Figure 2. a, b). There was neither lymphadenopathy nor metastasis on the first PET/CT. Six months after radiotherapy, the SUVmax decreased from 20.4 to 4 and there was also significant decrease in the size of tumor (Figure 2. c, d), (Table 1).
Case 3
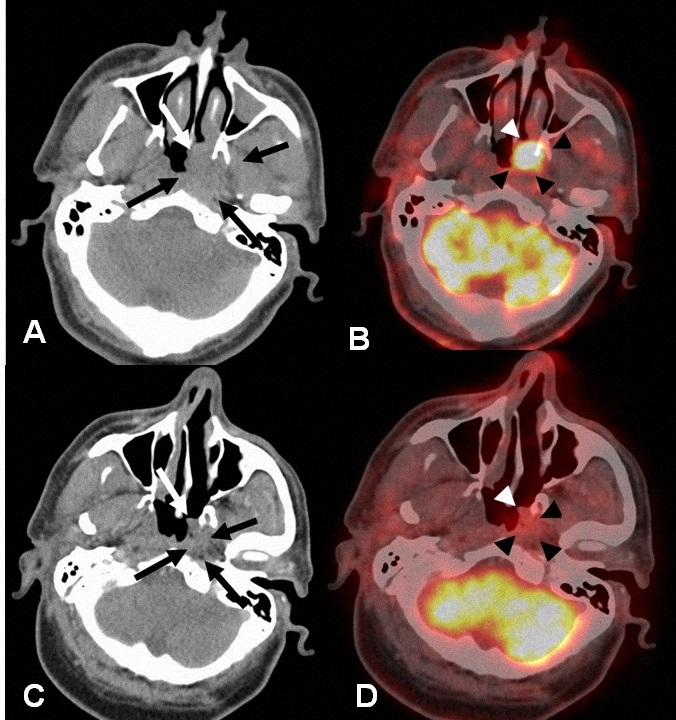
A 56-year-old male was admitted to our institution with the complaints of nasal congestion, occasional epistaxis and left sided loss of hearing, started 7 months before. Because a polypoid wall thickening in the left part of the nasopharynx, presumed to be nasopharynx cancer was observed during endoscopic examination, a biopsy was performed in the same session. The result was compatible with a nasopharyngeal plasmacytoma. On the initial PET/CT examination, a solid, nasopharyngeal mass with the extension of pterygopalatine fossa was seen (Figure 3. a, b). No additional FDG avid lesion was detected on the initial PET/CT. Six months after radiotherapy, the longest diameter as well as the SUVmax value declined significantly (Figure 3. c, d), (Table 1).
Case 4
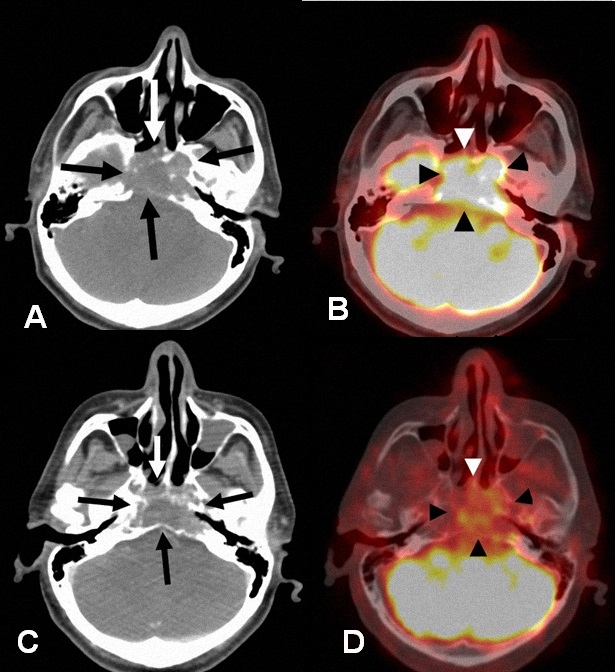
A 46-year-old man was referred to our institution with a deep-seated, persistent neck pain, started within the last six months. No palpable mass was detected in the neck during physical examination. The presumed diagnosis of a chordoma was thought due to the detection of a destructive mass of clivus on CT. However, the biopsy result was compatible with a plasmacytoma. Prior to radiotherapy, a destructive, lytic mass originating from clivus with the invasion of cavernous sinus and carotid artery was detected on PET/CT with a SUVmax of 14 (Figure 4. a, b). There was no dramatic change in the size of tumor after radiotherapy (Table 1), while the SUVmax of the mass decreased from 14 to 5.7 (Figure 4. c, d).
Discussion
The diagnostic criterias for extramedullary plasmacytoma (EMP) comprise; monoclonal plasma cell histology in tissue biopsy, less than 5% of plasma cell in bone marrow aspiration, lack of multiple lytic bone lesions supporting MM, absence of hypercalcemia, renal failure as well as high serum paraprotein levels 9, 10. Upper aerodigestive tract is the classic involvement region for EMP and the tumor often tends to involve HN region 11, 12. In a wide review, Alexiou et al. reviewed more than 400 articles and it is demonstrated that most of the EMPs (82.2%) originated from the upper aerodigestive tract, while 17.8% of EMPs originated from gastrointestinal tract, urogenital system, skin, lung and breast 11.
Cross-sectional imaging methods such as CT and MRI are helpful in diagnosis, evaluation of morphological characteristics of the tumor and also in determination of the extent of the disease. However, these modalities lack the determination of the metabolic status of the tumor and they are inadequate in evaluation of the treatment (e.g. radiotherapy) response. On the other hand PET/CT can effectively evaluate the treatment response. Although control PET/CT revealed no dramatic length reduction of the lesions in our first and fourth cases after radiotherapy, 84.5% and 59.2% FDG uptake reduction were detected, respectively. Regarding these two cases, we can conclude that the metabolic response occurs long time before the size reduction of tumor.
In a meta-analysis conducted by Lu et al. 14 distinct studies ( a total of 395 patients) were analyzed in order to find the effectiveness of PET/CT in extramedullary involvement of MM. As a result of this study, the sensitivity and specificity of PET/CT were found as 96% and 77.8%, respectively. The authors concluded that the whole-body PET/CT is a valuable imaging method in determination of extramedullary involvement 13.
In conclusion, PET/CT as a molecular imaging technique is superior in evaluation of HN plasmacytomas and in treatment response with regard to classic cross-sectional imaging modalities especially in the lesions without any size reduction of tumor after treatment. PET/CT has a further advantage of showing cartilage involvement as demonstrated in our fourth patient.
References
- International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003;121:749?7.
- Galieni P, et al. Solitary plasmacytoma of bone and extramedullary plasmacytoma: two different entities? Ann Oncol. 1995;6:687?91.
- Castro EB, Lewis JS, Strong EW. Plasmacytoma of paranasal sinuses and nasal cavity. Arch Otolaryngol. 1973;97:326-9.
- Ozdemir S, et al. A case of extramedullary plasmacytoma in the sphenoid sinus with unilateral loss of vision. J Craniomaxillofac Surg. 2013;41:140-3.
- Durie BG, Salmon SE. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer. 1975;36:842?54.
- Horger M, et al. Modern imaging techniques during therapy in patients with multiple myeloma. Acta Radiol. 2011;52:881-8.
- Hanrahan CJ, Christensen CR, Crim JR. Current concepts in the evaluation of multiple myeloma with MR imaging and FDG PET/CT. Radiographics. 2010;30:127?42.
- Shortt CP, et al. Whole-Body MRI versus PET in assessment of multiple myeloma disease activity. Am J Roentgenol. 2009;192:980?6.
- Galieni P, et al. Clinical outcome of extramedullary plasmacytoma. Haematologica. 2000;85:47-51.
- Liebross RH, et al. Clinical course of solitary extramedullary plasmacytoma. Radiother Oncol. 1999;52:245-9.
- Alexiou C, et al. Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer. 1999;85:2305?4.
- Soesan M, et al. Extramedullary plasmacytoma: clinical behaviour and response to treatment. Ann Oncol.1992;3:51?7.
- Lu YY, et al. FDG PET or PET/CT for detecting intramedullary and extramedullary lesions in multiple Myeloma: a systematic review and meta-analysis. Clin Nucl Med. 2012;37:833-7.
|