Abstract
Primary epiploic appendagitis is a rare disorder occuring as a result of the inflammation of the epiploic appendages of colon. Because it is self limiting and requires only conservative treatment, differential diagnosis from the other entities, which present with similar symptoms and need surgical intervention must be made. Computed tomography is the most efficient and accurate imaging modality for this purpose. Thus unnecessary surgery and use of antibiotics can be avoided.
Keywords :
Abdominal
, Epiploic
Turkish Abstract
Primer epiploik apendajit, nadir görülen ve kolonun epiploik apendikslerinin inflamasyonu sonucu oluşan bir durumdur. Kendi kendini sınırlaması ve konservatif tedavinin yeterli olması nedeniyle, cerrahi gerektiren ve benzer klinik bulgular gösteren diğer abdominal ağrı nedenlerinden ayırımı yapılmalıdır. Bunun için bilgisayarlı tomografi en etkin ve kesin sonuç veren görüntüleme yöntemidir. Bu sayede, gereksiz cerrahiden ve antibiyotik kullanımından kaçınılmış olur.
Turkish Keywords :
, Abdominal
, Epiploik
Introduction
Epiploic appendages are small outpouching sacs covered with serosa and filled with fat and localized in the tenia coli over the external surface. The number of these appandages is about 100, and their average size is about 3 cm 1. One or two small end arteries of vasa recta longa of the colon supply each appandage, and through its narrow pedicle passes the draining tortuous vein 2-4.
Primary epiploic appendagitis (PEA) is rare and presents with the inflammation of the epiploic appendages without the inflammation of adjacent structures. The cause is usually a spontaneous torsion, or a hemorrhagic infarct, etc 5-8.
PEA is a rarely encountered cause of localized abdominal pain. The accurate and the differential diagnosis of this situation is important, since the treatment is conservative and the patients can be saved from unnecessary surgical interventions. Because the clinical findings are similar to those requiring surgical treatment, radiology plays a major role in the management of the disease.
Here we present a case with epiploic appendagitis and its computed tomography(CT) findings.
Case Report
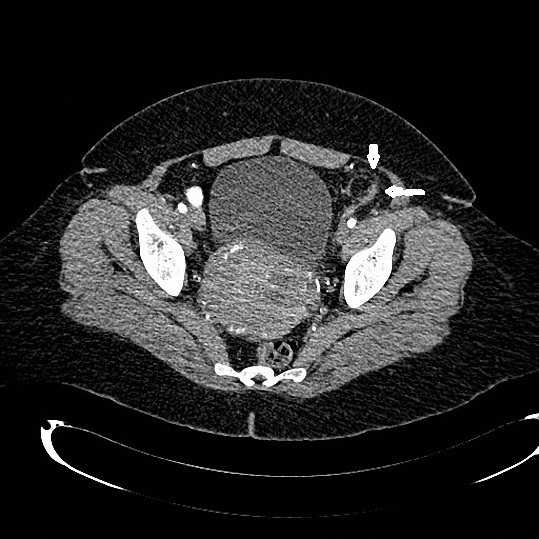
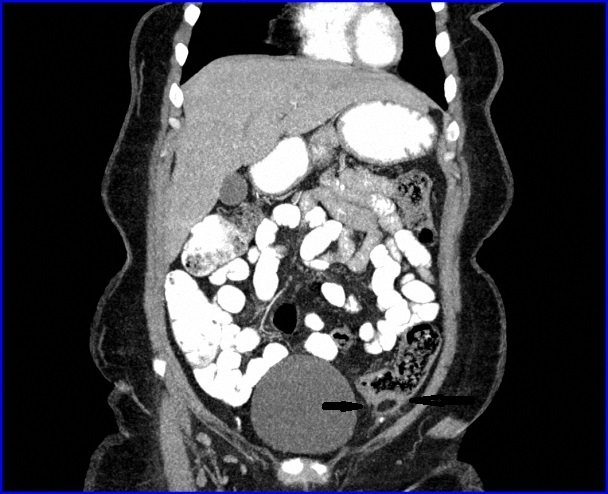
A 41 years old woman referred to our hospital with a left sided, sharp, non radiating,localized abdominal pain. It had an onset two days ago and was gradually worsening. She had a value of leukocyts as 9500 and CRP was 2,84.mg/L She did not have urinary symptoms or altering in bowel habits. She had a nonspesific ultrasound examination without a prediagnosis. Then she was directed to the tomography department to be scanned with CT, to enlighten the reason of unexplained abdominal pain. In CT images, a round fatty lesion with an enhancing surrounding rim was detected in the left iliac fossa.This lesion was anterior to the descending colon with a mesenteric stranding around. There was no sign of obstruction, diverticulitis or bowel wall thickening. And there were no inflammatory changes in the surrounding organs either. These imaging findings were consistent with primary epiploic appendagitis. The patient was admitted to the hospital for observation,and treatment with analgesics, anti inflammatory drugs, intraveneous fluid. With the improvement of clinical condititon and relieving of the complications overnight, she was discharged the other day with her treatment arranged as oral analgesia.
Discussion
Epiploic appendages are small pouches of peritoneum. They are filled with fat and small vessels that protrude from the serosal surface of the colon 9. They have been reported to act like cushions to support the colon and to be involved in immune functions, like a small omentum, and also in colonic absorption 10,11. Their limited blood supply, together with their pedunculated shape, make epiploic appendages prone to ischemic infarction 1,12,13.
Epiploic appendagitis may occur anywhere in the colon; mostly in rectosigmoid junction with 57% of cases as the literature suggests. The second site, we see 26% of the cases in the ileocecal region, then 9% in the ascending colon, 6% in the transverse colon and 2% in the descending colon. The incidence is higher in males and mostly occurs in the fourth and fifth decades 14-16.
PEA may mimic other disorders and present its symptoms according to its localization. But the main symptoms are non radiating and localized abdominal pain of rapid onset. In abdominal examination the abdomen is usually soft not distended, whereas shows a localized tenderness 9. The labaroraty tests are usually nonspesific and does not give enough information about the diagnosis. CT utilization is very helpful, with the identification of round or ovoid lesions of fatty density with a hyper attenuating rim which is the diagnostic hallmark and surrounding ill-defined fat stranding in the mesenteric fat adjacent to the colon 17 (Figure 1,2). This pathognomonic CT finding eliminates the need to perform an exploratory laparoscopy. Omental infarct can mimic PEA, but it has a bigger mass and generally located at right. Contrarily to PEA which is located to anterolateral of colon, omental infarct is found generally in the medial aspect of ascending and descending colon. Hyperattenuating rim and central spot can not be detected on CT 18. Also CT can easily differentiate other acute disorders presenting with lower abdominal pain like acute appendicitis, diverticulitis etc. which require surgical intervention.Clinical findings and localization help with differential diagnosis with acute appendicitis. A long segment of thickened bowel wall which we don?t observe in PEA is a typical finding for diverticulitis 18.
In a study made by Singh et al. 13 the CT findings have totally resolved in patients having a CT scan six months after the first presentation. Residual findings in the evolution of the PEA may be; decrease in size of the fatty core with increase in the overall density, decrease in size only, increase in overall density only, and mild residual stranding density in the mesocolon 13. PEA is a self limited situation and the treatment of PEA is conservative, usually with anti inflammatory drugs. Many clinicans are not familiar with this entity, but it must be a differential diagnosis to be regarded. With the improvement of cross-sectional imaging modalities and contribution of CT to the diagnosis, many patients have been saved from unnecessary surgery, antibiotic use or hospitalization 9,12,13.
References
- Blinder E, Ledbetter S, Rybicki F. Primary epiploic appendagitis. Emerg Radiol. 2002; 9: 231?334
- Sandrasegaran K, et al. Primary epiploic appendagitis: CT diagnosis. Emerg Radiol. 2004; 11: 9?14
- Sand M, et al. Epiploic appendagitis: clinical characteristics of an uncommon surgical diagnosis. BMC Surg. 2007; 1;7?11
- Jain T, et al. Primary epiploic appendagitis: radiological diagnosis can avoid surgery. Semin Roentgenol. 2008; 43: 4?6.
- Carmichael DH, Organ CH Jr. Epiploic disorders. Conditions of the epiploic appendages. Arch Surg. 1985;120:1167-72.
- Dockerty MB, Lynn TE, Waugh JM. A clinicopathologic study of the epiploic appendages. Surg Gynecol Obstet. 1956;103:423-33.
- Thomas JH, Rosato FE, Patterson LT. Epiploic appendagitis. Surg Gynecol Obstet.1974; 138: 23-5.
- Fieber SS, Forman J. Appendices epiploicae: clinical and pathological considerations: report of three cases and statistical analysis on one hundred five cases. AMA Arch Surg. 1953;66: 329-38.
- Hwang JA, et al. Differential diagnosis of left-sided abdominal pain: primary epiploic appendagitis vs colonic diverticulitis. World J Gastroenterol. 2013 28; 19(40):6842-8.
- Ross JA. Vascular loops in the appendices epiploicae; their anatomy and surgical significance, with a review of the surgical pathology of appendices epiploicae. Br J Surg.1950;37: 464-6.
- Vinson DR. Epiploic appendagitis: a new diagnosis for the emergency physician. Two case reports and a review. J Emerg Med. 1999; 17: 827-32
- Almeida AT, et al. Epiploic appendagitis: an entity frequently unknown to clinicians ? diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol. 2009; 193: 1243?51
- Singh AK, et al. Acute epiploic appendagitis and its mimics. Radiographics. 2005; 25: 1521?34
- Desai HP, et al. Infarction of an epiploic appendage. Review of the literature. J Clin Gastroenterol. 1993;16(4):323-325.
- Macari M, et al. Caecal epiploic appendagitis: an unlikely occurrence. Clin Radiol. 2008;63(8):895-900.
- Fraser J.D, et al. Infarction of an epiploic appengage in a pediatric patient. J. Pediatr. Surg. 2009;44, 1659-1661.
- Issa IA, Berjaoui MT, Hamdan WS. Primary epiploic appendagitis: from A to Z. Int Med. Case Rep J. 2010 22 (3): 67-9.
- Koplay M, et al. Primary epiploic appendagitis: Clinic and radiologic imaging findings. Dicle Med J. 2013; 40 (2): 264-268
|